Migraine Management in Pilots: A Focused Narrative Review for the Treating Neurologist
Article information

Abstract
Migraine, one of the leading global causes of disability, presents a complex challenge in aviation medicine. Headache is the fourth most common cause of in-flight pilot incapacitation, and cockpit-related exposures—including hypobaric hypoxia, low humidity, circadian disruption, and, in military aviation, sustained +Gz loading—may lower the migraine threshold. At the same time, aeromedical regulations restrict the medication options available to treating neurologists. This focused narrative review synthesizes pilot-specific clinical evidence and the principal regulatory documents issued by the International Civil Aviation Organization (ICAO Annex 1 and Doc 8984) and the U.S. Federal Aviation Administration (FAA Aviation Medical Examiner Guide) to provide neurologists with a practical framework for managing pilots with migraine. Simple analgesics, including acetaminophen/paracetamol, ibuprofen, naproxen, and aspirin at standard doses, are permitted under both ICAO and FAA frameworks. Triptans are permitted by the FAA after a 24- to 48-hour ground-observation period, whereas gepants such as ubrogepant and rimegepant require a 48-hour observation period. Beta-adrenergic blockers and calcium channel blockers are accepted preventive agents under both frameworks after a 7-day ground trial, whereas tricyclic antidepressants, topiramate, valproate, opioids, and butalbital-containing compounds are unacceptable. Anti–calcitonin gene-related peptide monoclonal antibodies are now accepted by the FAA after a 7-day ground trial, providing an additional certification-compatible option for pilots with migraine refractory to traditional preventive therapy. Most pilots with migraine can be managed in a manner compatible with continued flight duty when the neurologist selects medications within the applicable aeromedical formulary and documents clinical stability objectively to support certification.
INTRODUCTION
Migraine is a common and important cause of disability worldwide. The global age-standardised prevalence is approximately 14.1%.1 Although migraine can be severely disabling during an attack, it is regarded as a benign disorder that does not threaten life in most cases, and the therapeutic goals for most patients are symptom control during attacks and prevention of chronification.
Given this prevalence, a substantial proportion of commercial and military pilots also live with migraine. When the affected patient is a pilot, however, the problem extends beyond the conventional clinical setting. A migraine attack can in itself compromise the safe operation of an aircraft carrying hundreds of passengers; equally, several common migraine medications can reduce vigilance, slow psychomotor performance, or otherwise impair alertness. Even a slight decrement in cognitive function during a critical phase of flight can lead to a catastrophic accident. Migraine in pilots is therefore a matter of concern not only for the treating clinician but also for the aviation regulatory authorities responsible for flight safety.
The aviation environment itself can aggravate migraine. Pilots are repeatedly exposed to mild hypobaric hypoxia, irregular work–rest schedules, sleep deprivation, transmeridian travel, cosmic radiation at altitude, and the cumulative demands of long-haul operations—all recognised migraine triggers.2,3 These same exposures impose comparatively little symptomatic burden on most passengers and on cabin crew, but in the pilot the consequences differ in kind: even mild hypoxia that is well tolerated by passengers may trigger an attack, impair higher cognitive function, and degrade flight performance.
Most neurologists are not aviation medical examiners (AMEs), yet those who care for pilot patients must understand a key principle: certain migraine phenotypes and several commonly prescribed migraine medications are not permitted in pilots under the rules of the International Civil Aviation Organization (ICAO)4 and the U.S. Federal Aviation Administration (FAA), as further operationalised in the FAA Aviation Medical Examiner Guide.5,6 Because both the diagnosis itself and the prescriptions written to manage it can threaten a pilot’s medical certificate, pilots are often reluctant to seek medical attention; the disorder is consequently under-diagnosed and under-treated, and many affected pilots rely on over-the-counter analgesics alone.
This focused narrative review addresses migraine in the pilot patient from the dual perspective of clinical neurology and aeromedical certification, integrating the regulatory frameworks of the ICAO and FAA with the contemporary headache-medicine literature on triptans, gepants, and anti–calcitonin gene-related peptide (CGRP) monoclonal antibodies. Both civilian commercial pilots and military aviators are addressed.
This review is reported in accordance with the Scale for the Assessment of Narrative Review Articles (SANRA), which evaluates narrative reviews across six criteria: justification of the review’s importance, statement of concrete aims, description of the literature search, referencing, scientific reasoning, and presentation of data. Each criterion is addressed as follows: the clinical importance and aims of the review are stated in the Introduction; literature was identified through a structured search of PubMed from January 2000 to March 2026, supplemented by hand-searching reference lists of key articles and relevant grey literature, including regulatory documents from ICAO and the FAA. Search terms included combinations of the following: ‘migraine,’ ‘headache,’ ‘pilot,’ ‘aviator,’ ‘aviation,’ ‘aerospace medicine,’ ‘aeromedical,’ ‘flight,’ ‘CGRP’, ‘triptan,’ and ‘gepant.’ Articles were included if they addressed migraine epidemiology, clinical management, or aeromedical certification in civilian or military pilots, were written in English, and were published in peer-reviewed journals or as official regulatory documents. Case reports, editorials without original data, and articles addressing exclusively non-pilot populations were excluded. Given the limited volume of pilot-specific literature, a broad inclusion approach was adopted consistent with narrative review methodology.
EPIDEMIOLOGY AND UNDER-REPORTING OF MEDICAL CONDITIONS
Under-reporting of medical conditions in pilots is well recognised and is one of the most important confounders of any prevalence estimate in this population. In a Norwegian web-based survey, 9,941 applicants for an aeromedical certificate or attestation were invited and 1,616 responded; 188 of the respondents (12%) admitted to having under-reported at least one item of information—covering mental or physical health, medications, or drug use—and 50% of established pilots reported personal knowledge of a colleague who had under-reported.7
Reliable epidemiological data on migraine in pilots, and especially in commercial airline pilots, are therefore sparse. Fear of grounding, of loss of livelihood, and of stigma plausibly suppress migraine disclosure as much as they suppress disclosure of any other condition that might jeopardise medical certification. The treating neurologist should not assume that the migraine history obtained at consultation reflects the patient’s true symptomatic burden.
The most informative datasets come from military aviation. In an anonymous voluntary survey of 1,389 U.S. military officer trainees, the lifetime prevalence of migraine was 18% (14% in men and 31% in women); migraine had been previously diagnosed in only 10% of these trainees, and only 3% of those meeting diagnostic criteria for migraine had ever been prescribed a triptan. Eight per cent of trainees reported impairment of performance attributable to migraine during the training period.8
AVIATION ENVIRONMENT TRIGGERING MIGRAINE
Pilots in the aircraft cabin or cockpit are exposed to multiple recognised migraine triggers. Mild hypobaric hypoxia lowers arterial oxygen saturation by a few percentage points, slightly reduces cerebral arteriolar tone, and promotes the release of nitric oxide and CGRP—mechanisms that overlap with the trigeminovascular activation seen in both migraine and high-altitude headache.2,3
Cabin relative humidity of 10%–20% promotes mucosal dehydration and can precipitate migraine. Long-haul operations, night flying, transmeridian travel, sleep deprivation, and circadian misalignment all substantially lower the migraine threshold.4,9
In military aviation, sustained positive and negative Gz loading is an additional recognised cause of acute headache; this topic, however, is beyond the scope of the present review.
MIGRAINE CHARACTERISTICS AND FLIGHT DUTY
The diagnosis of migraine should be established according to the International Classification of Headache Disorders, 3rd edition (ICHD-3).10 When determining medical fitness, the assessor should focus on the seven factors enumerated in ICAO Doc 8984 §10.2.4: prodrome, precipitating factors, aura, rapidity of onset, attack frequency, severity, and therapy.4
Awareness of prodromal symptoms and identifiable precipitating factors is important because it allows avoidance, and a gradual onset over hours similarly permits in-flight avoidance manoeuvres, whereas onset within minutes does not. According to ICAO Doc 8984 §10.2.6, one or two attacks per year may not be disqualifying, while several attacks per month are likely to preclude certification.4 Importantly, ICAO does not specify fixed numerical thresholds; rather, it provides directional guidance and leaves the final certification determination to the individual aeromedical assessor’s judgement (§10.2.4, §10.2.6). This contrasts with the FAA Conditions Aviation Medical Examiners Can Issue (CACI) framework, which sets explicit quantitative criteria.
Aura is of disproportionate aeromedical importance. ‘A tiny scintillating or shimmering crescent in a small fraction of the visual field may be inconsequential, whereas transient loss of half of the visual field would be unquestionably compromising.’4 The instrument-flight environment is intolerant of even brief impairment of central vision, and a scintillating scotoma overlying a primary flight display can incapacitate a single-pilot operation. Sensory and dysphasic auras carry corresponding risks for radio communication. Hemiplegic migraine, migraine with brainstem aura, retinal migraine, and migrainous infarction warrant special concern and are excluded from the FAA CACI streamlined certification pathway.5,6
Triggers should be explicitly characterised as avoidable or unavoidable; unavoidable triggers—such as the stress and sleep deprivation intrinsic to the flying duty itself—substantially complicate the certification pathway.
Red flags for secondary headache mandate urgent neuroimaging. The threshold for magnetic resonance imaging in the pilot patient should be lower than in the general population, because missed secondary pathology has direct safety implications. A normal scan also has documentary value when later supporting a Special Issuance application.
The certification implications of the principal migraine phenotypes and clinical features under the ICAO and FAA frameworks are summarised in Table 1.
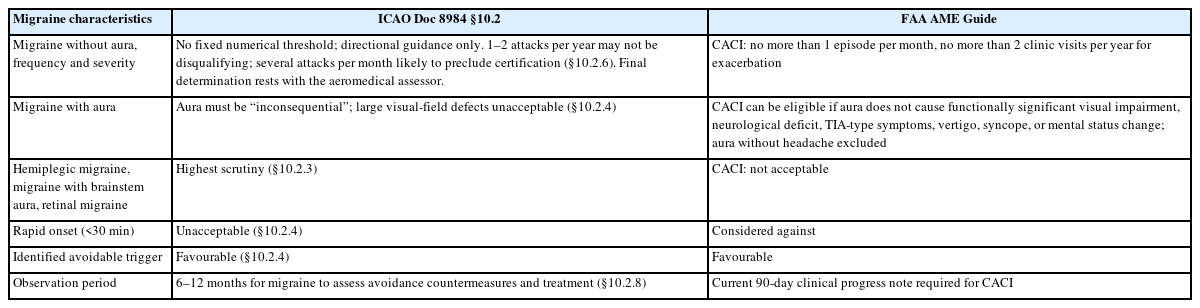
Certification implications of clinical characteristics of migraine in the ICAO and FAA frameworks
ACUTE TREATMENT COMPATIBLE WITH FLIGHT DUTY
Simple analgesics—paracetamol, ibuprofen, naproxen, and aspirin in standard doses—are permitted in the cockpit by both ICAO and FAA, provided that symptom control is adequate and the headache is not in itself incapacitating.4,5 They should generally be tried before escalation to triptans or gepants, because demonstrated effectiveness with a simple agent simplifies certification.
The FAA Guide for Aviation Medical Examiners permits short-acting triptans (sumatriptan, naratriptan, zolmitriptan, almotriptan, rizatriptan) with a mandatory 24-hour ground-observation period after each dose; eletriptan and frovatriptan, with longer half-lives, require 72 hours.6,11 The treating neurologist should always document the agent, the time of dose, and the pilot’s tolerance for the certifying authority’s record.
Gepants—small-molecule CGRP receptor antagonists—are an emerging class with a more favourable cardiovascular profile than triptans and no ergot-like vasoconstriction. The FAA accepts ubrogepant and rimegepant with a 48-hour observation period after each dose.6,11 Gepants’ rapid onset (30 to 45 minutes) makes them theoretically attractive for use well before flight if a prodromal warning is recognised, although this practice is not yet endorsed by any aeromedical authority and would require ground confirmation of tolerance.
Lasmiditan, a 5-HT1F agonist, carries a U.S. Food and Drug Administration–mandated 8-hour driving restriction owing to demonstrable cognitive and psychomotor impairment; it is currently accepted by the FAA only on a Special Issuance conditional basis. Antiemetic adjuncts are constrained: metoclopramide is acceptable to the FAA with a 36-hour observation period; promethazine is sedating and requires a 96-hour FAA observation period.6,11
Opioids and butalbital-containing compounds (e.g., Fioricet, Fiorinal) are unacceptable under both the ICAO and FAA frameworks, with the small ICAO caveat that low-dose codeine (15 mg every 6 hours) is regarded as ‘probably safe’ under §14.44 of Doc 8984.4,5 Ergot alkaloids occupy a more nuanced position under the FAA framework: dihydroergotamine and ergotamine are accepted under CACI with post-dose observation periods of 48 and 24 hours respectively.6 ICAO Doc 8984 does not provide migraine-specific guidance on ergot alkaloids; however, §14.3.13 classifies dihydroergotamine alkaloids among sympatholytic agents associated with postural hypotension, bradycardia, sedation, weakness, and mental confusion, and §14.3.15 characterises this pharmacological class as generally unsuitable for active flight crew. The absence of a corresponding ICAO entry in Table 2 therefore reflects not regulatory silence but the absence of condition-specific guidance within a broader framework that is unfavourable to this drug class. Newer dihydroergotamine precision olfactory delivery systems such as INP104 have similarly demonstrated a favourable cardiovascular safety profile in non-aviation populations.12 Table 2 summarises the position of each authority on the principal acute migraine medications.
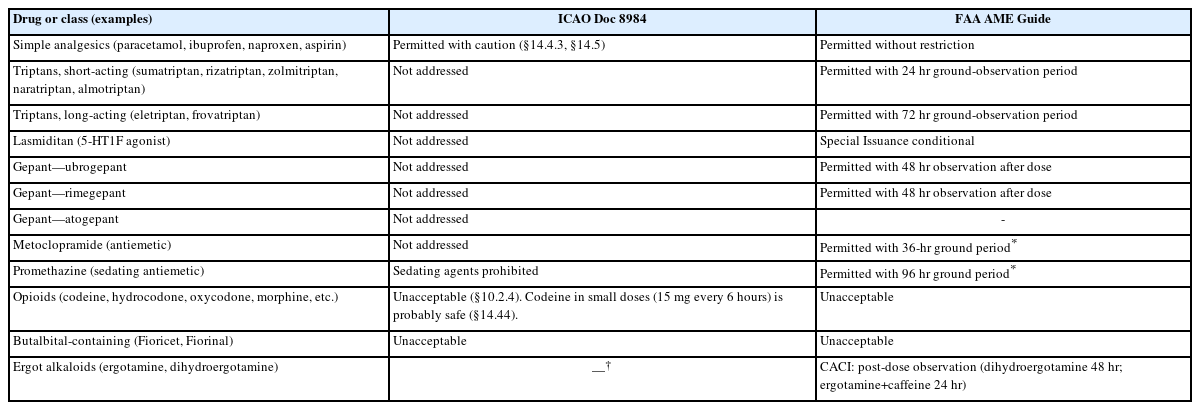
Aeromedical acceptability of acute migraine medications under the ICAO and FAA frameworks
PREVENTIVE TREATMENT COMPATIBLE WITH FLIGHT DUTY
When attack frequency or severity warrants prophylaxis, agent selection in the pilot must integrate clinical evidence with aeromedical acceptability. Beta-adrenergic blockers (propranolol, metoprolol, nadolol) are accepted as first-line preventives by both ICAO and FAA, provided that no clinically significant bradycardia or hypotension is present and a 7-day ground trial—a mandatory period of off-flight-duty observation to confirm tolerability and freedom from adverse effects before the pilot returns to aviation duties—confirms tolerance.4-6 Calcium channel blockers, particularly flunarizine, are similarly accepted under the same conditions.
Tricyclic antidepressants (amitriptyline, nortriptyline)—including at low migraine-prophylactic doses—are not acceptable under either the ICAO or FAA frameworks for migraine prophylaxis, reflecting the broader caution about antidepressants articulated in ICAO Doc 8984: ‘antidepressants … preclude their use in aviators.’4 Selective serotonin reuptake inhibitors (SSRIs) are considered with similar caution under §14.4.22 of the same Manual; FAA acceptance of individual SSRIs and serotonin–norepinephrine reuptake inhibitor is conditional and varies by agent.4,6
Topiramate—the most commonly prescribed preventive in the general migraine population—is unacceptable under both the ICAO and FAA frameworks because of its effects on cognitive processing speed and word-finding.4,5,6,11 ICAO Doc 8984 §10.2.6 lists ‘anticonvulsants’ generically as unacceptable, and valproate and other anticonvulsants share this status. The pilot patient previously stabilised on topiramate frequently presents to the neurologist seeking an alternative regimen that will permit recertification—a clinical scenario for which the anti-CGRP class is now of considerable importance.
1. Anti–calcitonin gene-related peptide monoclonal antibodies and the changing regulatory landscape
Erenumab, fremanezumab, galcanezumab, and eptinezumab—monoclonal antibodies targeting the CGRP ligand or receptor—are now recommended preventive options for migraine under contemporary international guidelines, including the 2022 European Headache Federation update.13 They are highly effective, generally well tolerated, and largely devoid of the central-nervous-system side-effect profile that has historically grounded pilots on traditional preventives. Real-world adherence rates are several-fold higher than for oral preventives.
FAA acceptance of CGRP monoclonal antibodies for migraine prophylaxis has expanded materially since approximately 2020; these agents are now permitted under FAA guidance after a 7-day ground trial confirms efficacy and absence of adverse effects.6,11 ICAO Doc 8984, last revised in 2012, predates this class entirely. For pilot patients with chronic or high-frequency episodic migraine who cannot tolerate or qualify for traditional preventives, anti-CGRP therapy may now be the single most important pathway to restored fitness for duty, and this is arguably the most important practical change in the aeromedical migraine landscape in two decades.
OnabotulinumtoxinA for chronic migraine prevention is accepted by the FAA on a Special Issuance conditional basis, with awareness of potential delayed adverse effects; individual evaluation is the rule.6 Behavioural interventions—biofeedback, cognitive-behavioural therapy, structured sleep hygiene, regular aerobic exercise, and trigger-avoidance counselling—carry no aeromedical concern and should constitute the foundation of every pilot’s preventive regimen. Table 3 summarises the position of each authority on the principal preventive migraine medications.
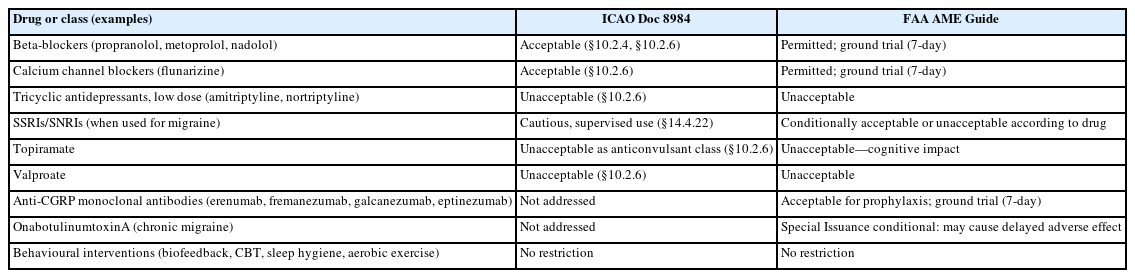
Aeromedical acceptability of preventive migraine medications under the ICAO and FAA frameworks
THE AEROMEDICAL CERTIFICATION FRAMEWORK EXPLAINED
Migraine certification operates within a two-tier international hierarchy. ICAO Annex 1 §6.3.2.3 establishes the international Standard that no Class 1 applicant ‘shall have any … progressive or non-progressive disease of the nervous system, the effects of which are likely to interfere with the safe exercise of the applicant's licence and rating privileges.’14 ICAO Doc 8984 Part III, Chapter 10 then provides the detailed clinical guidance, applying the so-called ‘1% rule’: any condition conferring greater than 1% annual risk of sudden incapacitation is incompatible with safety-sensitive aviation duty.4 National authorities operationalise these principles; the FAA Aviation Medical Examiner Guide provides the most detailed publicly available implementation framework relevant to neurologists managing migraine in pilots.5,6
1. Federal Aviation Administration—the Conditions Aviation Medical Examiners Can Issue pathway
Since April 2013 the FAA has permitted Aviation Medical Examiners to issue medical certificates directly under the CACI programme for migraine and chronic headache. The principal certification criteria include the following: the condition must be stable on the current regimen with no recommended medication changes; symptoms must be mild and non-disabling; headache frequency must not exceed one episode per month; and none of the following disqualifying features may be present: auras without headache, functionally significant visual impairment, neurological impairment, transient ischemic attack (TIA)-type symptoms, vertigo, syncope, or mental status change.5,6 Pilots not meeting CACI criteria require Special Issuance Authorisation through the FAA Aerospace Medical Certification Division. Migraine with aura, hemiplegic migraine, retinal migraine, and complicated migraines with TIA-type symptoms are all excluded from CACI and require special issuance.
2. Military pilots
Military aviation medical regulators—the U.S. Air Force (USAF), U.S. Navy, Royal Air Force, and others—operate aeromedical waiver programmes that share the conceptual framework of civilian authorities but apply substantially stricter criteria, particularly for combat aviation. Migraine with neurological aura, hemiplegic migraine, basilar migraine, and any migrainous event during high-G manoeuvres typically warrant permanent disqualification from fighter operations, although waivers for non-combat or transport platforms remain possible.15,16 The USAF outcome data of Hesselbrock and Haynes15—91% retention of certification at long-term follow-up after waiver—offer a strong empirical basis for cautious optimism in carefully selected military aviators with well-controlled migraine.
PRACTICAL CONSIDERATIONS AND RETURN-TO-FLY
Effective management of the pilot patient with migraine requires the treating neurologist to assemble a defensible documentary record. Helpful elements include: a contemporaneous headache diary capturing date, time, duration, severity, aura features, identified trigger, medication used, and time to symptom resolution; a clear ICHD-3 diagnostic statement; a current pharmacological regimen with documentation of efficacy and absence of side-effects on the aeromedically acceptable formulary; and a recent normal neuroimaging study where any atypical features were present.
Communication with the pilot is itself a clinical intervention. Pilots are well-served by an explicit acknowledgement of the disclosure dilemma and by clear advice that contemporary regulatory pathways—particularly in the U.S.—now accommodate well-managed migraine. The neurologist should resist the temptation to prescribe restricted medications under the assumption that ‘the pilot will not fly when symptomatic’; agents on the do-not-issue/do-not-fly list (opioids, butalbital, ergots, topiramate, valproate) jeopardise certification regardless of the prescriber’s intent.
Operational risk mitigation should be discussed proactively. Multi-pilot operations afford a measure of fail-safe coverage that single-pilot operations do not. After any acute migraine episode, a return-to-fly decision should be made jointly by the treating neurologist, the AME, and—when certification status is uncertain—the licensing authority, with documentation of full symptom resolution, no medication side-effects, and an attack-free interval consistent with regulatory expectations (typically 6 to 12 months under ICAO Doc 8984 §10.2.8 for migraine).4
A limitation of the present review is that we focused on the ICAO and FAA regulatory frameworks, as these provide the most detailed and publicly accessible pharmacological guidance. Most other non-U.S. jurisdictions rely on ICAO principles but do not publish equivalent drug-specific lists. The regulatory recommendations presented here should therefore be interpreted in the context of the applicable national authority for each pilot patient.
A further limitation is that the evidence supporting the use of anti-CGRP monoclonal antibodies and gepants in pilots derives primarily from general migraine trials; no prospective studies have evaluated flight-performance outcomes or aeromedical safety endpoints in pilot populations receiving these agents. This evidence gap reinforces the importance of close collaboration between the treating neurologist, the AME, and the licensing authority throughout the certification process.
Regulatory guidance in aviation medicine is subject to ongoing revision as the evidence base expands. All drug acceptability and observation period requirements cited in this review reflect FAA and ICAO documents current as of March 2026; clinicians are strongly encouraged to consult the most recent version of the relevant authority’s guidance before advising pilot patients.
CONCLUSION
Migraine in pilots is a clinically common, regulatorily complex, and operationally significant condition. The treating neurologist’s task is no longer simply to control headache; it is to restore and maintain the pilot’s medical certification while doing so. Most pilots with infrequent, predictable, well-controlled migraine without significant aura can be managed compatibly with continued flight duty under contemporary ICAO and FAA frameworks.
The regulatory acceptance of anti-CGRP monoclonal antibodies and gepants represents a meaningful step forward for pilots with migraine refractory to conventional preventives, given their favourable cognitive side-effect profile compared with topiramate or amitriptyline. However, it should be noted that pilot-specific real-world evidence and long-term aviation safety data for these agents remain limited; clinical experience to date is largely extrapolated from general migraine prevention trials. Neurologists are therefore advised to document objective evidence of tolerability and absence of side-effects carefully and to remain vigilant for any emerging aeromedical safety signals as post-marketing experience grows.
Effective collaboration among neurologist, AME, and licensing authority remains the single most important determinant of clinical and operational success.
Notes
AVAILABILITY OF DATA AND MATERIAL
Not applicable. All data discussed are derived from previously published, publicly accessible sources cited in the references.
AUTHOR CONTRIBUTIONS
Conceptualization: KYP; Formal analysis: KYP; Investigation: CYP, DK, HL, HBJ, KYP; Methodology: KYP; Writing–original draft preparation: CYP, KYP; Writing–review & editing: CYP, DK, HL, HBJ, KYP.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING STATEMENT
None.
ACKNOWLEDGMENTS
None.