The Hidden Risks of Medication Underuse in Migraine Progression
Article information

Abstract
Migraine is a progressive neurological disorder in which inadequate treatment can lead to chronification. For decades, clinical attention has centered on medication overuse headache (MOH) as the primary iatrogenic risk factor for this progression. However, medication underuse (MU) has emerged as a critical yet less established framework for understanding gaps in migraine care. This review reframes MU, which includes ineffective therapies, delayed administration, and non-adherence due to intolerability, as an active contributor to disease progression. Untreated or undertreated migraine attacks promote the development of central sensitization, a state of neuronal hyperexcitability that increases attack frequency, severity, and treatment resistance. This paper posits that MU and MOH are not opposing concepts but interconnected manifestations of suboptimal disease management. Specifically, disease progression driven by MU can directly precipitate the escalating medication use that characterizes MOH, resulting in a more refractory clinical state. Therefore, preventing chronification requires a paradigm shift from merely avoiding overuse to achieving optimal use. This entails adherence to evidence-based guidelines for both acute and preventive therapy—implementing stratified acute care within the neurobiological window to prevent central sensitization and initiating timely preventive treatment in eligible patients to reduce the overall attack burden. The integration of novel targeted therapies provides new opportunities to overcome the limitations of traditional agents. Ultimately, reducing the risks associated with MU through proactive, evidence-based management and strong patient–clinician communication is essential to alter the natural history of migraine and prevent the long-term disability associated with its progression.
INTRODUCTION
Migraine is a highly prevalent neurological disorder, affecting approximately 12%–15% of the global adult population and representing the leading cause of disability in individuals under 50 years of age.1 The condition imposes a significant burden, leading to impaired quality of life, reduced productivity, and substantial socioeconomic costs from both direct healthcare expenditures and indirect losses.2 Migraine is not a static condition but a progressive disorder, with an estimated 2.5% of individuals with episodic migraine transitioning to chronic migraine (CM) annually.3 This progression highlights the need for effective management strategies to mitigate its extensive personal and societal impact.
Current standard treatments include acute therapies for rapid symptom relief and preventive regimens to reduce attack frequency and severity. The prompt and appropriate application of these medications is fundamental to achieving favorable outcomes and preventing chronification.4 However, a pivotal and often underrecognized issue in clinical practice is medication underuse (MU), defined as the suboptimal application of indicated treatments, including underutilization, poor adherence, delayed administration, or premature discontinuation.5 Such underuse can aggravate migraine progression by permitting the neuroplastic changes, such as central sensitization, that amplify attack frequency, intensity, and treatment resistance.6
The hidden risks of MU include an increased likelihood of chronification, exacerbation of comorbid conditions, and greater healthcare demands, which are often overshadowed by the clinical emphasis on medication overuse headache (MOH). This review investigates the complex relationship between MU and migraine progression, highlighting its foundational risks and advocating for proactive clinical interventions. Subsequent sections will outline the mechanisms of underuse, its clinical impact, and evidence-based guidelines for optimized care, with the goal of mitigating these underappreciated risks.
PATHOPHYSIOLOGY OF MIGRAINE CHRONIFICATION
1. Central sensitization as a core mechanism
Central sensitization is a key neurophysiological phenomenon underlying migraine chronification.7 It refers to a state of hyperexcitability in central pain-transmitting neurons, particularly in the trigeminocervical complex and thalamus, induced by persistent and intense nociceptive input.8 In this state, the activation threshold of neurons is lowered, leading to responses to stimuli that are normally not painful and to spontaneous neuronal firing.
Clinically, central sensitization manifests as allodynia, where innocuous stimuli, such as combing hair or light touch, are perceived as painful.9 When migraine attacks are recurrent and inadequately treated, the intense afferent signals from the peripheral trigeminal system induce neuroplastic changes that alter synaptic strength in central neurons.10 This activity-dependent process establishes a persistent state of hypersensitivity in the pain system, creating a vicious cycle of increased attack frequency, greater intensity, and diminished treatment response. Thus, CM should be understood not merely as frequent headaches but as a disease state characterized by chronic sensitization of the central nervous system.
2. The role of neuropeptides and neuroinflammation
Neuropeptides, particularly calcitonin gene-related peptide (CGRP), and subsequent neurogenic inflammation play a pivotal role in migraine attacks and chronification.11 During a migraine attack, CGRP is released in large quantities from activated trigeminal nerve endings.12 The released CGRP acts on dural blood vessels, causing vasodilation, and stimulates mast cells to release inflammatory mediators such as histamine and serotonin.13
This cascade triggers a localized, sterile inflammatory response in the dura mater, which in turn stimulates trigeminal nerve endings, creating a positive feedback loop that amplifies pain signals.14 Each inadequately treated migraine attack represents a significant inflammatory event that provides a powerful afferent stimulus, promoting and maintaining central sensitization. The cumulative effect of these repeated, uncontrolled inflammatory processes can induce long-term changes in central pain circuits, thereby facilitating the transition to CM.15 This highlights that the goal of migraine therapy should extend beyond simple pain relief to the rapid and effective termination of the underlying neuroinflammatory process.
THE ROLE OF MEDICATION OVERUSE IN MIGRAINE PROGRESSION
For decades, MOH has been the most prominent iatrogenic factor in the study and clinical management of migraine chronification.16 Considered the “best-documented iatrogenic factor in migraine chronification,” MOH is a secondary headache disorder caused by the excessive use of acute headache medications.17 The International Classification of Headache Disorders (ICHD)-3 defines MOH as the worsening of a pre-existing headache or the development of a new type of headache in the context of regular overuse of specific medications for more than 3 months.18 The core pathophysiology of MOH is a vicious cycle. To manage escalating headaches, patients increase their intake of acute medication. The medication overuse itself then disrupts the brain’s endogenous pain modulation systems, lowering the headache threshold and increasing headache frequency (Figure 1).19 This leads patients to consume even more medication to treat the worsening pain. This cycle is thought to involve complex biological mechanisms, including neurotransmitter receptor downregulation, dysfunction of endogenous pain control systems, and exacerbation of central sensitization.20 Furthermore, behavioral and psychological factors, such as anticipatory anxiety and pain-related fear, can reinforce medication dependency and perpetuate the cycle.21
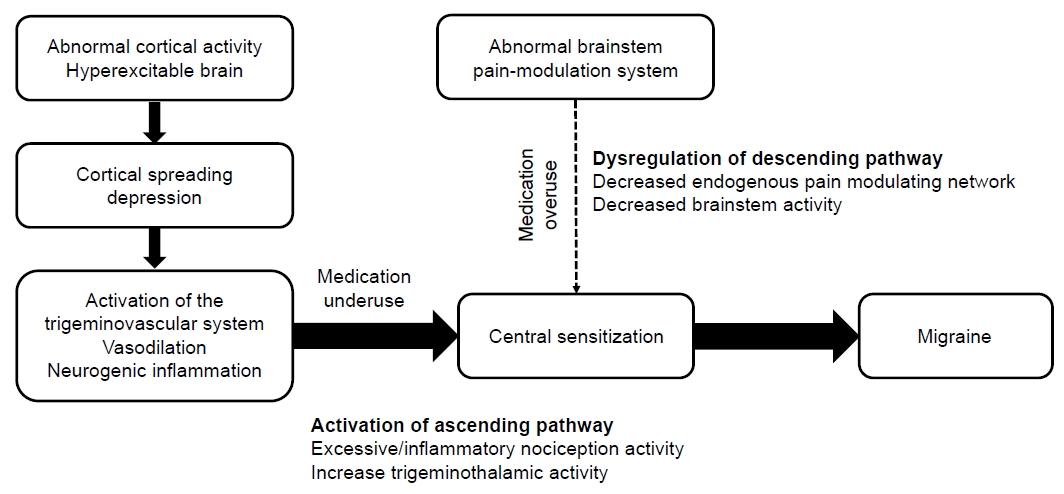
Interplay of medication underuse and overuse in migraine progression.
The identification of MOH and research into its mechanisms have led to significant advances in migraine care. Warning patients about its risks is an essential component of patient safety. As a result, MOH has become a central topic in clinical guidelines, patient education, and academic research for decades.22 Clinicians worldwide now consider it standard practice to instruct patients to track their acute medication use and adhere to established limits. These efforts have undoubtedly prevented many patients from developing MOH. However, this intense focus on MOH has created a consequential oversight in clinical paradigms. Clinical discourse regarding medication use has concentrated almost exclusively on the dangers of using “too much,” while the potential risks of using “too little” have been relatively neglected. The powerful message that frequent use of acute medication is dangerous has framed the conversation around restriction and regulation. Consequently, there has been a lack of systematic investigation into the negative impact of failing to use appropriate medication when needed—a phenomenon termed MU on migraine progression.5 This has created a paradoxical situation where the system designed to prevent one iatrogenic problem (MOH) may inadvertently contribute to another: disease progression due to MU.
A PARADIGM SHIFT: INVESTIGATING MEDICATION UNDERUSE AS A CATALYST FOR PROGRESSION
1. Defining and quantifying medication underuse
MU is a multidimensional concept that encompasses several distinct patterns of suboptimal treatment. These include the ineffective utilization of appropriate therapies, where a medication is not well-matched to attack severity, leading to prolonged headache exposure and heightened risk of central sensitization.5,23 It also involves underutilization among eligible patients, where a significant proportion of individuals who warrant acute or preventive therapy do not receive it, contributing to disease progression.24,25 Another critical aspect is the inappropriate timing of administration, particularly delaying acute medication until an attack is severe, which significantly reduces efficacy by failing to halt the propagation of central sensitization.5,26 Finally, patient dissatisfaction, stemming from insufficient efficacy or intolerable side effects, often leads to non-adherence or premature discontinuation of therapy, which are major factors in poor adherence for both acute and preventive medications.25,27 Objectively measuring these dimensions presents methodological challenges, requiring a comprehensive approach that utilizes patient diaries, prescription data, and validated questionnaires to quantify the patterns and extent of underuse.28
2. Key manifestations of acute medication underuse
The underuse of acute medication is a critical iatrogenic factor in migraine progression, manifesting primarily through inadequate treatment efficacy, suboptimal prescribing and delayed administration, and poor tolerability leading to non-adherence.5 Suboptimal efficacy is a principal contributor to chronification. The American Migraine Prevalence and Prevention (AMPP) Study found a direct, graded association between poor treatment response and the risk of new-onset CM, with individuals reporting “very poor” efficacy having 2.55 times the odds of progressing compared to those with “maximal” efficacy.23 This is mirrored in South Korean claims data, where extremely high discontinuation rates for acute therapies—with only 25.2% of new triptan users persisting after three months—suggest a significant issue with perceived efficacy or tolerability.29
The timing of medication intake also profoundly influences therapeutic success. Contemporary paradigms favor immediate treatment at headache inception to prevent the establishment of central sensitization.5 The TEMPO study demonstrated that early triptan administration (<1 hour post-onset) yielded significantly higher rates of 2-hour pain freedom compared to late administration (≥1 hour).30 Furthermore, suboptimal prescribing contributes to underuse. In South Korea, for instance, newly diagnosed migraine patients are most frequently prescribed non-steroidal anti-inflammatory drugs (NSAIDs) (69.9%) or acetaminophen (50.0%), rather than migraine-specific triptans, which may be inadequate for moderate-to-severe attacks.29 Lastly, poor tolerability is a major barrier to effective treatment. Data from the Chronic Migraine Epidemiology and Outcomes (CaMEO) Study revealed that 35.5% of individuals who had ever used acute prescription medications had discontinued them, with tolerability (24.9%) and efficacy concerns (28.2%) being key reasons.31 The challenge of non-adherence is starkly illustrated in South Korea, where 65.7% of newly diagnosed patients discontinue their initial acute treatment within 3 months, highlighting a critical gap in maintaining effective therapy.29
3. Key manifestations of preventive medication underuse
Underuse of preventive medication represents a significant gap in migraine care, leaving many patients vulnerable to disease progression. This issue is influenced by low initiation rates among eligible patients, poor adherence, and high discontinuation rates for those who start therapy, and challenges with tolerability. A substantial proportion of individuals who meet established criteria for preventive therapy do not receive it. In the United States, it is estimated that while approximately 38% of people with migraine qualify for prophylaxis, only 12%–13% actually use it.32,33 This treatment gap is a global issue, with European data showing that only 26% of eligible patients use traditional preventive agents, and a South Korean analysis finding that only 7.3% of newly diagnosed patients were prescribed preventive treatment.29,34
Even when preventive therapy is initiated, adherence and persistence are notably poor, particularly with traditional oral agents. Real-world data report adherence rates as low as 17%–20% at 12 months, with persistence even lower in CM populations.35,36 Data from South Korea mirror these findings, showing persistence rates for some preventive treatments dropping to just 6%–7% after 12 months.29 A primary factor in this low adherence is the adverse effect profile of many traditional preventive medications. Meta-analyses show that approximately 23% of patients withdraw from clinical trials due to side effects, and in real-world settings, tolerability concerns contribute to discontinuation in up to 30% of cases.37,38 This dissatisfaction is a key factor leading to treatment abandonment, which perpetuates a cycle of underuse and leaves patients exposed to the risks of migraine progression.39
4. Etiology of underuse
MU is a complex behavior resulting from the interplay of psychological, educational, and socioeconomic factors. These can be broadly categorized into patient-centered barriers and system- or clinician-related barriers. Patient-centered barriers include fear of side effects, which many find more distressing than the headache itself, and concerns about addiction or tolerance, which may be an unintended consequence of warnings about MOH.21,40 Distrust in efficacy from past negative experiences can also lower expectations for new treatments, while social stigma may cause patients to avoid taking medication in public.27,41
System- and clinician-related barriers are also significant. Limited access to care, due to geographic distance or long wait times, can prevent timely management.24 The high cost of newer, more effective treatments is another substantial barrier that can cause patients to ration or forgo medication.42 Finally, insufficient clinician education can lead to a failure to adequately address patient fears and misconceptions or to provide clear instructions, resulting in a passive or hesitant approach to treatment on the part of the patient.43
5. A hypothesized mechanism for underuse-mediated progression
The central hypothesis of this review is that underuse of acute migraine medication is causally linked to the progression to CM. The proposed biological mechanism involves a cascade beginning with the repetition of uncontrolled neuroinflammation. When a migraine attack is untreated or undertreated, the release of CGRP and subsequent neurogenic inflammation persist at maximum intensity and for a prolonged duration (Figure 1).11 This potent and sustained inflammatory state strongly stimulates trigeminal nerve endings, sending a massive barrage of nociceptive signals to the central nervous system.8 The repeated transmission of these intense pain signals acts as a powerful stimulus that strengthens synaptic connections and lowers activation thresholds in the trigeminocervical complex and thalamus, effectively inducing and consolidating a state of central sensitization.9 At the clinical level, these neurobiological changes manifest as an increased frequency and severity of headache attacks, diminished responsiveness to future treatments, and ultimately, the transformation to CM.5 In summary, MU accelerates chronification by sustaining ascending nociception and eroding descending inhibition, underscoring the need for timely pharmacotherapy to preserve neural homeostasis.
MU and overuse are not mutually exclusive phenomena; rather, they can interact dynamically within a patient’s disease course. A patient might initially adopt an underuse strategy due to fears of MOH and side effects. This underuse could promote disease progression and deepen central sensitization, making headaches more frequent and severe. Faced with intractable pain, the patient may then overcome their initial fears and begin using medication frequently out of desperation, transitioning into a state of overuse. This suggests that underuse is not merely the opposite of overuse, but can be a direct precursor, facilitating the disease progression that culminates in the frequent medication use characteristic of MOH. To emphasize the relationship between MU and MOH, Table 1 summarizes their key features including definitions, behaviors, pathophysiological mechanisms, clinical consequences, and management strategies, emphasizing their interconnected roles in disease progression.
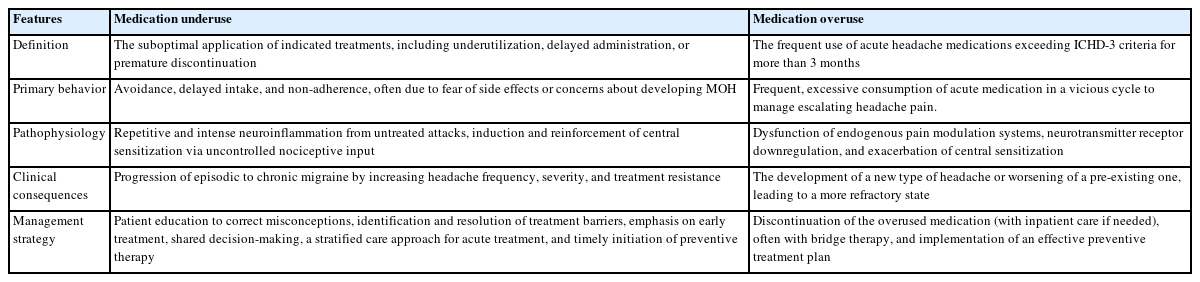
Comparative analysis of medication overuse and underuse in migraine progression
CLINICAL IMPLICATIONS AND A NEW FRAMEWORK FOR MIGRAINE MANAGEMENT
1. Re-evaluating the therapeutic window
The primary goal of acute migraine treatment is rapid pain cessation, ideally within 2 hours, to halt the underlying neuroinflammatory cascade and prevent attack recurrence.44 Effective and timely treatment is critical because a migraine attack is a progressive neurological event. The development of cutaneous allodynia—pain from normally non-painful stimuli—serves as a clinical marker for the establishment of central sensitization.8 This process follows a distinct timeline: within 1 hour of headache onset, allodynia may appear on the same side as the pain; by 2 hours, it can spread to the opposite side of the head and even the limbs, indicating that sensitization has progressed from second- to third-order neurons in the thalamus.8 This neurobiological cascade creates a critical therapeutic window. Preclinical and clinical studies demonstrate that early intervention can block central sensitization, whereas delayed treatment is significantly less effective. For example, the response rate to sumatriptan is 93% in non-allodynic patients but only 15% in those who have already developed allodynia.8 Therefore, optimal use of acute medication is not merely for symptomatic relief but is a crucial strategy to prevent the neuroplastic changes that facilitate treatment resistance and disease progression.
2. Acute treatment guidelines to prevent underuse
To prevent the underuse that facilitates chronification, clinical guidelines advocate for a stratified care approach, which tailors therapy to attack severity rather than employing a step care model.45 This strategy is more effective and cost-efficient in reducing disability. For mild attacks, NSAIDs are recommended as initial therapy. For moderate to severe attacks, migraine-specific agents, triptans are first-line. Triptans should be administered at an adequate dose early in the attack, ideally within 60 minutes of onset, to optimize efficacy and prevent central sensitization.5 If the initial response is inadequate, options include combining a triptan with an NSAID or switching to an alternative triptan, as individual responses can vary. For patients in whom triptans are ineffective, poorly tolerated, or contraindicated due to cardiovascular risk, newer classes of medication, such as gepants (ubrogepant, rimegepant) or lasmiditan are recommended.45,46 These agents provide effective alternatives without the vasoconstrictive properties of triptans. Patient education is crucial to prevent MOH, limiting simple analgesics, NSAIDs, or lasmiditan to fewer than 10 days per month, and combined analgesics or triptans to 8 days per month. Gepants may be preferable in individuals at higher risk for MOH, as there is currently no evidence linking gepants to MOH.46
3. Preventive treatment guidelines to prevent underuse
Preventive therapy is a cornerstone of migraine management, aimed at reducing attack frequency, severity, and duration, which in turn decreases reliance on acute medications and lowers the risk of both underuse and overuse.47 Prophylaxis is indicated for patients with 4 or more monthly headache days, significant disability despite acute treatment, or contraindications to acute therapies. To combat underuse, guidelines recommend selecting first-line agents with high-level evidence, such as beta-blockers, certain anticonvulsants, and CGRP-targeted therapies.48,49 Treatment should be initiated at a low dose and titrated slowly to improve tolerability and prevent premature discontinuation. A crucial element to prevent underuse is allowing an adequate trial period before judging efficacy: at least 2 to 3 months for oral agents at a target dose, and 3 to 6 months for injectable therapies. If a treatment is ineffective or poorly tolerated, switching to an agent from a different class is recommended over abandonment of preventive strategy.
4. The role of novel targeted therapies in addressing underuse
The advent of CGRP-targeted therapies, including monoclonal antibodies (mAbs) and gepants, has significantly advanced migraine prevention by offering superior efficacy and tolerability compared to many traditional oral agents.45 Their targeted mechanism results in higher response rates and fewer systemic side effects, which can improve adherence and persistence. Consequently, recent guidelines endorse anti-CGRP mAbs as a potential first-line option, removing the requirement to fail multiple older medications first.45 However, significant barriers contribute to their underuse. High costs and restrictive reimbursement policies often limit access to patients with refractory migraine who have failed several other treatments.34 For example, in South Korea, reimbursement for CGRP mAbs is restricted to patients with CM who have failed at least three oral preventives.29 This is problematic, as a higher number of prior treatment failures is a negative predictor of response to anti-CGRP therapy.50 Emerging evidence on response predictors such as lower baseline headache frequency and good response to triptans suggests that earlier initiation of these targeted therapies may optimize outcomes and prevent the progression of disease burden.
CONCLUSION
Migraine is a progressive neurological disorder, but its progression is often preventable. This review repositions MU not as a passive failure of treatment but as an active, iatrogenic risk factor for migraine chronification. The long-held clinical focus on MOH has, while important, overshadowed the reality that underuse and overuse are two facets of the same core problem: suboptimal disease management. Ineffective or delayed acute treatment allows for the establishment of central sensitization, which increases headache frequency and reduces therapeutic response.5 This, in turn, can lead patients toward more frequent medication intake, creating a direct pathway from underuse to overuse and a more refractory disease state.23
Halting this progression requires a paradigm shift toward optimal use, guided by evidence-based principles. This includes the timely and effective application of acute therapies within the critical neurobiological window to prevent central sensitization, and the early consideration of preventive therapy for eligible patients to reduce the overall attack burden. A crucial component of this strategy is the ongoing assessment of treatment efficacy and tolerability, fostering a collaborative relationship between clinician and patient to identify and overcome barriers to adherence. Educating both healthcare providers and patients on the profound risks of underuse is paramount. By treating each migraine attack effectively and implementing preventive strategies proactively, it is possible to alter the natural history of the disease, prevent the cycle of underuse and overuse, and mitigate the long-term disability associated with CM.
Notes
AVAILABILITY OF DATA AND MATERIAL
The data presented in this study are available upon reasonable request from the corresponding author.
AUTHOR CONTRIBUTIONS
Conceptualization: HSM, PWC; Writing–original draft: HSM; Writing–review & editing: HSM, PWC.
CONFLICT OF INTEREST
Heui Soo Moon received honoraria as a moderator/speaker/advisor from Abbvie Korea, Teva-Handok, Lundbeck Korea, Pfizer Korea, Oganon Korea, Dong-A Pharm, YuYu Pharm, SK Pharm, and Ildong Pharm. She was a site investigator for a multicenter trial sponsored by Biohaven Pharmaceuticals, Allergan Korea, and Ildong Pharmaceutical Company. She has received lecture honoraria from Eli Lilly and Company, Handok-Teva, and Ildong Pharmaceutical Company over the past 24 months. The other author has no other conflicts of interest to declare.
FUNDING STATEMENT
Not applicable.
ACKNOWLEDGMENTS
Not applicable.