
Articles
- Page Path
- HOME > Headache Pain Res > Volume 26(3); 2025 > Article
-
Review Article
The Hidden Risks of Medication Underuse in Migraine Progression -
Heui-Soo Moon
 , Pil-Wook Chung
, Pil-Wook Chung -
Headache and Pain Research 2025;26(3):209-217.
DOI: https://doi.org/10.62087/hpr.2025.0019
Published online: October 23, 2025
Department of Neurology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
- Correspondence: Pil-Wook Chung, M.D. Department of Neurology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, 29 Saemunan-ro, Jongno-gu, Seoul 03181, Republic of Korea Tel: +82-2-2001-2050, Fax: +82-2-2001-2049, E-mail: chungpw@hanmail.net
© 2025 The Korean Headache Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,354 Views
- 93 Download
- 3 Crossref
Abstract
- Migraine is a progressive neurological disorder in which inadequate treatment can lead to chronification. For decades, clinical attention has centered on medication overuse headache (MOH) as the primary iatrogenic risk factor for this progression. However, medication underuse (MU) has emerged as a critical yet less established framework for understanding gaps in migraine care. This review reframes MU, which includes ineffective therapies, delayed administration, and non-adherence due to intolerability, as an active contributor to disease progression. Untreated or undertreated migraine attacks promote the development of central sensitization, a state of neuronal hyperexcitability that increases attack frequency, severity, and treatment resistance. This paper posits that MU and MOH are not opposing concepts but interconnected manifestations of suboptimal disease management. Specifically, disease progression driven by MU can directly precipitate the escalating medication use that characterizes MOH, resulting in a more refractory clinical state. Therefore, preventing chronification requires a paradigm shift from merely avoiding overuse to achieving optimal use. This entails adherence to evidence-based guidelines for both acute and preventive therapy—implementing stratified acute care within the neurobiological window to prevent central sensitization and initiating timely preventive treatment in eligible patients to reduce the overall attack burden. The integration of novel targeted therapies provides new opportunities to overcome the limitations of traditional agents. Ultimately, reducing the risks associated with MU through proactive, evidence-based management and strong patient–clinician communication is essential to alter the natural history of migraine and prevent the long-term disability associated with its progression.
INTRODUCTION
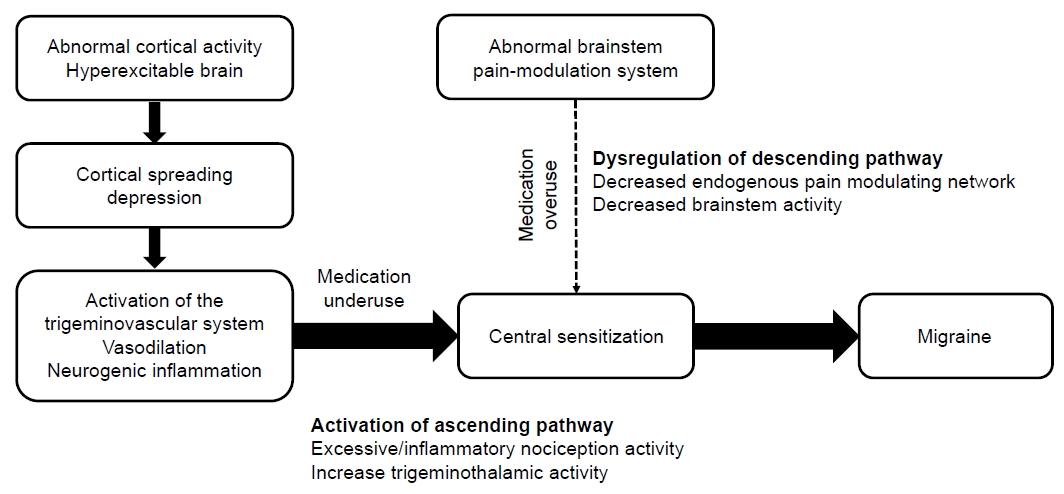
PATHOPHYSIOLOGY OF MIGRAINE CHRONIFICATION
THE ROLE OF MEDICATION OVERUSE IN MIGRAINE PROGRESSION
A PARADIGM SHIFT: INVESTIGATING MEDICATION UNDERUSE AS A CATALYST FOR PROGRESSION
CLINICAL IMPLICATIONS AND A NEW FRAMEWORK FOR MIGRAINE MANAGEMENT
CONCLUSION
AVAILABILITY OF DATA AND MATERIAL
The data presented in this study are available upon reasonable request from the corresponding author.
AUTHOR CONTRIBUTIONS
Conceptualization: HSM, PWC; Writing–original draft: HSM; Writing–review & editing: HSM, PWC.
CONFLICT OF INTEREST
Heui Soo Moon received honoraria as a moderator/speaker/advisor from Abbvie Korea, Teva-Handok, Lundbeck Korea, Pfizer Korea, Oganon Korea, Dong-A Pharm, YuYu Pharm, SK Pharm, and Ildong Pharm. She was a site investigator for a multicenter trial sponsored by Biohaven Pharmaceuticals, Allergan Korea, and Ildong Pharmaceutical Company. She has received lecture honoraria from Eli Lilly and Company, Handok-Teva, and Ildong Pharmaceutical Company over the past 24 months. The other author has no other conflicts of interest to declare.
FUNDING STATEMENT
Not applicable.
ACKNOWLEDGMENTS
Not applicable.
- 1. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020;396:1204-1222.ArticlePubMedPMC
- 2. Edmeads J, Mackell JA. The economic impact of migraine: an analysis of direct and indirect costs. Headache 2002;42:501-509.ArticlePubMedPDF
- 3. Bigal ME, Lipton RB. Modifiable risk factors for migraine progression. Headache 2006;46:1334-1343.ArticlePubMed
- 4. Ornello R, Caponnetto V, Ahmed F, et al. Evidence-based guidelines for the pharmacological treatment of migraine, summary version. Cephalalgia 2025;45:3331024251321500.ArticlePubMed
- 5. Rattanawong W, Rapoport A, Srikiatkhachorn A. Medication “underuse” headache. Cephalalgia 2024;44:3331024241245658.ArticlePubMedPDF
- 6. Mungoven TJ, Henderson LA, Meylakh N. Chronic migraine pathophysiology and treatment: a review of current perspectives. Front Pain Res (Lausanne) 2021;2:705276.ArticlePubMedPMC
- 7. Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain 2011;152:S2-S15.ArticlePubMedPMC
- 8. Burstein R, Cutrer MF, Yarnitsky D. The development of cutaneous allodynia during a migraine attack clinical evidence for the sequential recruitment of spinal and supraspinal nociceptive neurons in migraine. Brain 2000;123:1703-1709.ArticlePubMed
- 9. Suzuki K, Suzuki S, Shiina T, Kobayashi S, Hirata K. Central sensitization in migraine: a narrative review. J Pain Res 2022;15:2673-2682.ArticlePubMedPMCPDF
- 10. Dodick D, Silberstein S. Central sensitization theory of migraine: clinical implications. Headache 2006;46 Suppl 4:S182-S191.ArticlePubMed
- 11. Ho TW, Edvinsson L, Goadsby PJ. CGRP and its receptors provide new insights into migraine pathophysiology. Nat Rev Neurol 2010;6:573-582.ArticlePubMedPDF
- 12. Goadsby PJ, Edvinsson L, Ekman R. Vasoactive peptide release in the extracerebral circulation of humans during migraine headache. Ann Neurol 1990;28:183-187.ArticlePubMed
- 13. Durham PL. Calcitonin gene-related peptide (CGRP) and migraine. Headache 2006;46 Suppl 1:S3-S8.ArticlePubMedPMC
- 14. Geppetti P, Capone JG, Trevisani M, Nicoletti P, Zagli G, Tola MR. CGRP and migraine: neurogenic inflammation revisited. J Headache Pain 2005;6:61-70.ArticlePubMedPMCPDF
- 15. Bigal ME, Lipton RB. The differential diagnosis of chronic daily headaches: an algorithm-based approach. J Headache Pain 2007;8:263-272.ArticlePubMedPMCPDF
- 16. Diener HC, Limmroth V. Medication-overuse headache: a worldwide problem. Lancet Neurol 2004;3:475-483.ArticlePubMed
- 17. Kristoffersen ES, Lundqvist C. Medication-overuse headache: epidemiology, diagnosis and treatment. Ther Adv Drug Saf 2014;5:87-99.ArticlePubMedPMCPDF
- 18. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018;38:1-211.ArticlePubMedPDF
- 19. De Felice M, Ossipov MH, Porreca F. Update on medication-overuse headache. Curr Pain Headache Rep 2011;15:79-83.ArticlePubMedPMCPDF
- 20. Srikiatkhachorn A, Tarasub N, Govitrapong P. Effect of chronic analgesic exposure on the central serotonin system: a possible mechanism of analgesic abuse headache. Headache 2000;40:343-350.ArticlePubMed
- 21. Saper JR, Da Silva AN. Medication overuse headache: history, features, prevention and management strategies. CNS Drugs 2013;27:867-877.ArticlePubMedPDF
- 22. Vandenbussche N, Laterza D, Lisicki M, et al. Medication-overuse headache: a widely recognized entity amidst ongoing debate. J Headache Pain 2018;19:50.ArticlePubMedPMCPDF
- 23. Lipton RB, Fanning KM, Serrano D, Reed ML, Cady R, Buse DC. Ineffective acute treatment of episodic migraine is associated with new-onset chronic migraine. Neurology 2015;84:688-695.ArticlePubMedPMC
- 24. Diamond S, Bigal ME, Silberstein S, Loder E, Reed M, Lipton RB. Patterns of diagnosis and acute and preventive treatment for migraine in the United States: results from the American Migraine Prevalence and Prevention study. Headache 2007;47:355-363.ArticlePubMed
- 25. Buse DC, Sakai F, Matharu M, et al. Characterizing gaps in the preventive pharmacologic treatment of migraine: multi-country results from the CaMEO-I study. Headache 2024;64:469-481.ArticlePubMed
- 26. Wiley AT, Watson JC, Lehmann DN. Acute migraine headache: treatment strategies. Am Fam Physician 2025;111:317-327.PubMed
- 27. Hepp Z, Bloudek LM, Varon SF. Systematic review of migraine prophylaxis adherence and persistence. J Manag Care Pharm 2014;20:22-33.ArticlePubMedPMC
- 28. Buse DC, Lipton RB, Hallström Y, et al. Migraine-related disability, impact, and health-related quality of life among patients with episodic migraine receiving preventive treatment with erenumab. Cephalalgia 2018;38:1622-1631.ArticlePubMedPDF
- 29. Kim KY, Ko HY, Bea S, Lee HJ, Shin JY, Chu MK. Treatment patterns and persistence among patients newly diagnosed with migraine in South Korea: a retrospective analysis of health claims data. J Clin Neurol 2024;20:529-536.ArticlePubMedPMCPDF
- 30. Lantéri-Minet M, Mick G, Allaf B. Early dosing and efficacy of triptans in acute migraine treatment: the TEMPO study. Cephalalgia 2012;32:226-235.ArticlePubMedPDF
- 31. Lipton RB, Hutchinson S, Ailani J, et al. Discontinuation of acute prescription medication for migraine: results from the Chronic Migraine Epidemiology and Outcomes (CaMEO) study. Headache 2019;59:1762-1772.ArticlePubMedPMCPDF
- 32. Lipton RB, Bigal ME, Diamond M, et al. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology 2007;68:343-349.ArticlePubMed
- 33. Ha H, Gonzalez A. Migraine headache prophylaxis. Am Fam Physician 2019;99:17-24.PubMed
- 34. Pascual J, Panni T, Dell’Agnello G, Gonderten S, Novick D, Evers S. Preventive treatment patterns and treatment satisfaction in migraine: results of the OVERCOME (EU) study. J Headache Pain 2023;24:88.ArticlePubMedPMCPDF
- 35. Hepp Z, Dodick DW, Varon SF, Gillard P, Hansen RN, Devine EB. Adherence to oral migraine-preventive medications among patients with chronic migraine. Cephalalgia 2015;35:478-488.ArticlePubMedPDF
- 36. Hepp Z, Dodick DW, Varon SF, et al. Persistence and switching patterns of oral migraine prophylactic medications among patients with chronic migraine: a retrospective claims analysis. Cephalalgia 2017;37:470-485.ArticlePubMedPMCPDF
- 37. Jackson JL, Cogbill E, Santana-Davila R, et al. A comparative effectiveness meta-analysis of drugs for the prophylaxis of migraine headache. PLoS One 2015;10:e0130733.ArticlePubMedPMC
- 38. Pringsheim T, Davenport WJ, Becker WJ. Prophylaxis of migraine headache. CMAJ 2010;182:E269-E276.ArticlePubMedPMC
- 39. Ornello R, Andreou AP, De Matteis E, Jürgens TP, Minen MT, Sacco S. Resistant and refractory migraine: clinical presentation, pathophysiology, and management. EBioMedicine 2024;99:104943.ArticlePubMedPMC
- 40. Rimmele F, Müller B, Becker-Hingst N, et al. Medication adherence in patients with cluster headache and migraine: an online survey. Sci Rep 2023;13:4546.ArticlePubMedPMCPDF
- 41. Young WB, Park JE, Tian IX, Kempner J. The stigma of migraine. PLoS One 2013;8:e54074.ArticlePubMedPMC
- 42. Bloudek LM, Stokes M, Buse DC, et al. Cost of healthcare for patients with migraine in five European countries: results from the International Burden of Migraine Study (IBMS). J Headache Pain 2012;13:361-378.ArticlePubMedPMCPDF
- 43. Matsuzawa Y, Lee YSC, Fraser F, et al. Barriers to behavioral treatment adherence for headache: an examination of attitudes, beliefs, and psychiatric factors. Headache 2019;59:19-31.ArticlePubMedPMCPDF
- 44. Puledda F, Sacco S, Diener HC, et al. International Headache Society global practice recommendations for the acute pharmacological treatment of migraine. Cephalalgia 2024;44:3331024241252666.ArticlePubMed
- 45. Ailani J, Burch RC, Robbins MS; Board of Directors of the American Headache Society. The American Headache Society Consensus Statement: update on integrating new migraine treatments into clinical practice. Headache 2021;61:1021-1039.ArticlePubMedPDF
- 46. Moon HS, Chung PW, Kim BK. New targeted drugs for acute treatment of migraine. Korean J Headache 2023;24:56-65.
- 47. Silberstein SD, Holland S, Freitag F, et al. Evidence-based guideline update: pharmacologic treatment for episodic migraine prevention in adults: report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology 2012;78:1337-1345.ArticlePubMedPMC
- 48. Puledda F, Sacco S, Diener HC, et al. International Headache Society global practice recommendations for preventive pharmacological treatment of migraine. Cephalalgia 2024;44:3331024241269735.ArticlePubMed
- 49. Ryu S. Beyond the pain: rethinking migraine care with the RELIEF PLAN approach. Headache Pain Res 2025;26:1-2.ArticlePDF
- 50. Hong JB, Lange KS, Overeem LH, Triller P, Raffaelli B, Reuter U. A scoping review and meta-analysis of anti-CGRP monoclonal antibodies: predicting response. Pharmaceuticals (Basel) 2023;16:934.ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Pediatric Headache in Korea: Beyond a Common Complaint to a Chronic Neurological Condition
Yun Jin Lee
Headache and Pain Research.2026; 27(1): 4. CrossRef - Finding the Sweet Spot between Medication Overuse and Underuse in Headache Medicine
Hong-Kyun Park
Headache and Pain Research.2026; 27(2): 96. CrossRef - Real-world effectiveness and safety of CGRP monoclonal antibodies in elderly migraine patients: a Korean multicenter study
Soohyun Cho, Mi-Kyoung Kang, Heui-Soo Moon, Mi Ji Lee, Soo-Kyoung Kim, Hong-Kyun Park, Woo-Seok Ha, Min Kyung Chu, Young-Eun Gil, Byung-Su Kim, Soo-Jin Cho
The Journal of Headache and Pain.2026;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-

- Related articles
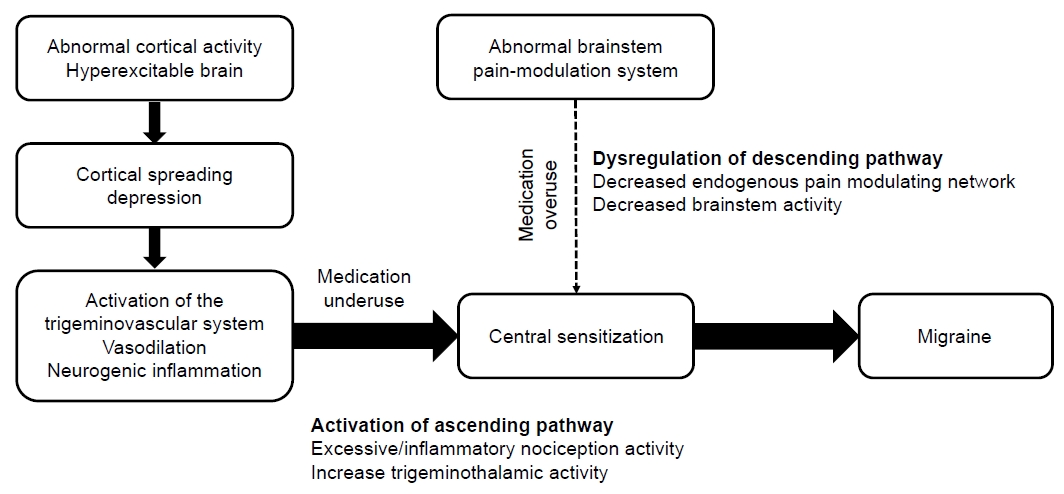
Figure 1.
| Features | Medication underuse | Medication overuse |
|---|---|---|
| Definition | The suboptimal application of indicated treatments, including underutilization, delayed administration, or premature discontinuation | The frequent use of acute headache medications exceeding ICHD-3 criteria for more than 3 months |
| Primary behavior | Avoidance, delayed intake, and non-adherence, often due to fear of side effects or concerns about developing MOH | Frequent, excessive consumption of acute medication in a vicious cycle to manage escalating headache pain |
| Pathophysiology | Repetitive and intense neuroinflammation from untreated attacks, induction and reinforcement of central sensitization via uncontrolled nociceptive input | Dysfunction of endogenous pain modulation systems, neurotransmitter receptor downregulation, and exacerbation of central sensitization |
| Clinical consequences | Progression of episodic to chronic migraine by increasing headache frequency, severity, and treatment resistance | The development of a new type of headache or worsening of a pre-existing one, leading to a more refractory state |
| Management strategy | Patient education to correct misconceptions, identification and resolution of treatment barriers, emphasis on early treatment, shared decision-making, a stratified care approach for acute treatment, and timely initiation of preventive therapy | Discontinuation of the overused medication (with inpatient care if needed), often with bridge therapy, and implementation of an effective preventive treatment plan |
ICHD, International Classification of Headache Disorders; MOH, medication overuse headache.
Table 1.
TOP

