Trigeminal Neuralgia: Pathophysiology, Clinical Features, and Therapeutic Management
Article information

Abstract
Trigeminal neuralgia (TN) is a severe, disabling neuropathic facial pain disorder classified among cranial neuralgias within headache medicine. Despite well-established diagnostic criteria, TN remains frequently misdiagnosed, particularly in dental and primary care settings. This review provides a clinically focused overview of the epidemiology, pathophysiology, classification, diagnostic approach, and contemporary management of TN, with relevance to headache and pain research and clinical practice. Neurovascular compression with focal demyelination at the trigeminal nerve root entry zone is considered the predominant mechanism in classical TN. Diagnosis is primarily clinical and guided by International Classification of Headache Disorders, 3rd edition criteria, with magnetic resonance imaging essential for excluding secondary and idiopathic causes. Carbamazepine and oxcarbazepine remain first-line therapies, whereas microvascular decompression and minimally invasive neurosurgical procedures provide effective options for medically refractory disease. TN requires accurate diagnosis and individualized management. Advances in pharmacological and interventional treatments have improved outcomes and underscore the importance of multidisciplinary care within headache and pain medicine.
INTRODUCTION
Trigeminal neuralgia (TN) is classified in the International Classification of Headache Disorders, third edition (ICHD-3), as a cranial neuralgia and represents one of the most severe forms of neuropathic facial pain encountered in clinical practice.1
TN is a chronic neuropathic pain disorder characterized by sudden, unilateral, brief episodes of severe, stabbing, or electric shock-like facial pain within the distribution of one or more branches of the trigeminal nerve. Historically referred to as tic douloureux, the condition has been recognized for centuries but remains a diagnostic and therapeutic challenge in contemporary clinical practice.2
Although relatively uncommon, TN exerts a disproportionate impact on quality of life because of the severity and unpredictability of pain attacks. Misdiagnosis is frequent, particularly in dental and primary care settings, often leading to unnecessary dental procedures and delayed neurological referral. A clearer understanding of TN pathophysiology, classification, and management is therefore essential to facilitate timely diagnosis and effective treatment.
EPIDEMIOLOGY
TN predominantly affects individuals over 50 years of age and shows a female predominance, with a female-to-male ratio of approximately 1.5–1.7:1. Although most cases are sporadic, TN can also occur as a secondary headache of neurological disorders such as multiple sclerosis or intracranial tumors.3 Despite its substantial psychological burden and impact on quality of life, epidemiological data remain limited, and the reported prevalence and incidence varies geographically.4 The estimated lifetime prevalence ranges from 0.16% to 0.3%.5 Due to the difference the prevalence (4-13) and lack of reference in the first sentence from the following sentences (25.33). A systematic review and meta-regression analysis conducted over a 79-year period (1945–2024) reported a pooled global incidence of 25.33 per 100,000 person-years (95% confidence interval [CI], 11.87–54.02; I2=99.96%; 95% prediction interval, 2.14–299.14), a pooled annual prevalence of 45.38 per 100,000 population (95% CI, 15.41–133.61; I2=98.76%; 95% prediction interval, 2.80–731.92), and a lifetime prevalence of 108.43 per 100,000 inhabitants (95% CI, 30.54–384.18). The analysis also reported a higher prevalence among females, right-sided predominance, and predominant involvement of the maxillary (V2) division. Region-specific estimates indicated the highest prevalence in Asia, particularly West Asia (98.50 [57.39–157.66]) and East Asia (85.76 [85.19–86.32]). Incorporation of neuroimaging into diagnostic criteria was associated with higher reported prevalence (84.98 [74.66–96.73]) compared with the pre-imaging era (7.98 [3.45–15.73]), suggesting that improved diagnostic methods contribute to earlier and more frequent detection.4 Given the increasing incidence among aging populations, improved awareness, and evolving diagnostic criteria, TN is not consistently considered a rare disorder due to variability in incidence across populations, although incidence rates continue to vary across populations.5
PATHOPHYSIOLOGY
The pathophysiology of TN is complex and involves genetic, structural, and neurobiological factors. Familial cases suggest a possible genetic predisposition.5 The prevailing mechanism in classical TN is neurovascular compression of the trigeminal nerve root entry zone, most commonly by the superior cerebellar artery. Chronic pulsatile compression leads to focal demyelination of primary trigeminal sensory neurons, resulting in abnormal impulse generation, neuroplastic changes, and ephaptic transmission between adjacent nerve fibers. These alterations render the nerve hyperexcitable, allowing otherwise innocuous stimuli to trigger paroxysmal pain.5 Familial TN is uncommon but has been reported, often presenting with right-sided facial pain involving the maxillary (V2) division. Rare ion channel gene variants identified in familial cases suggest potential genetic contributions, particularly affecting neuronal excitability. These findings highlight the value of further genomic investigation targeting neuronal excitability-related genes to better understand disease mechanisms.6 Structural and functional neuroimaging studies in patients with TN may reveal abnormalities in brain regions involved in pain modulation and emotional processing.7
Secondary TN arises from identifiable structural or demyelinating lesions, including multiple sclerosis plaques, tumors, vascular malformations, or brainstem infarctions. Central sensitization and cortical reorganization have also been implicated, particularly in patients with long-standing or refractory disease.1,7
CLINICAL FEATURES
TN is characterized by recurrent paroxysms of severe facial pain lasting from a fraction of a second to 2 minutes. The pain is typically described as intense, brief, sudden, stabbing, or electric shock-like and is often triggered by innocuous stimuli such as light touch, eating, speaking, tooth brushing, or exposure to cold air. As attack frequency increases, patients may become unable to perform routine daily activities. Some individuals avoid eating or speaking due to their fear of triggering pain episodes. Over time, this can markedly reduce quality of life and adversely affect mental well-being.2,5,7
Pain most commonly affects the maxillary (V2) or mandibular (V3) divisions of the trigeminal nerve. Attacks are typically separated by refractory periods, although some patients experience concomitant continuous background pain. Neurological examination is usually normal in classical TN; however, the presence of sensory deficits should prompt evaluation for secondary causes.8
CLASSIFICATION AND DIAGNOSTIC CRITERIA
The ICHD-3 categorizes TN into classical, secondary, and idiopathic forms. Diagnosis is primarily clinical and based on characteristic pain features, stimulus sensitivity, and exclusion of alternative causes. Magnetic resonance imaging (MRI) is recommended in all patients to identify neurovascular compression and exclude secondary pathology.1
Classical TN is diagnosed in patients with recurrent, sudden episodes of unilateral facial pain consistent with TN in whom MRI or surgical findings demonstrate true neurovascular compression, rather than simple contact, accompanied by structural changes such as nerve atrophy or displacement. These structural changes support the diagnosis. Compression most commonly occurs at the trigeminal nerve root entry zone, and arterial compression is more strongly associated with symptoms than venous compression. MRI can assess nerve volume and cross-sectional area, and atrophic changes may correlate with demyelination and neuronal loss. When identified preoperatively, these changes may predict a favorable response to microvascular decompression (MVD). The condition typically has an abrupt onset and most commonly affects the second or third division of the trigeminal nerve. Bilateral involvement is rare and usually occurs sequentially rather than simultaneously. Some patients experience a preceding phase of continuous atypical pain (pre-TN). Between attacks, most patients are symptom-free, although a subtype includes persistent background pain.1
Secondary TN is diagnosed in patients with recurrent unilateral facial pain consistent with TN, occurring either as brief attacks alone or in association with persistent background pain, when an underlying condition known to cause the neuralgia is identified. The diagnosis requires that the symptoms are not better accounted for by another ICHD-3 disorder. Recognized causes include tumors in the cerebellopontine angle, arteriovenous malformations, and multiple sclerosis. MRI is the preferred imaging modality for identifying an underlying cause. In patients who cannot undergo MRI, additional investigations, such as neurophysiological studies of trigeminal reflexes and trigeminal evoked potentials, may be used.
Idiopathic TN is diagnosed when neuroimaging studies, such as MRI, demonstrate contact between a blood vessel and the trigeminal nerve or its root but show no structural changes, such as nerve atrophy or displacement. Although this type of vascular contact is commonly observed in healthy individuals, the absence of morphological abnormalities means that the criteria for classical TN are not met (Table 1, 2).1
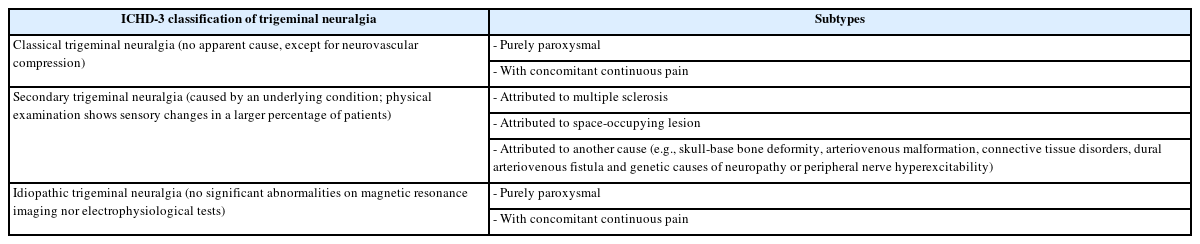
ICHD-3 classification of trigeminal neuralgia
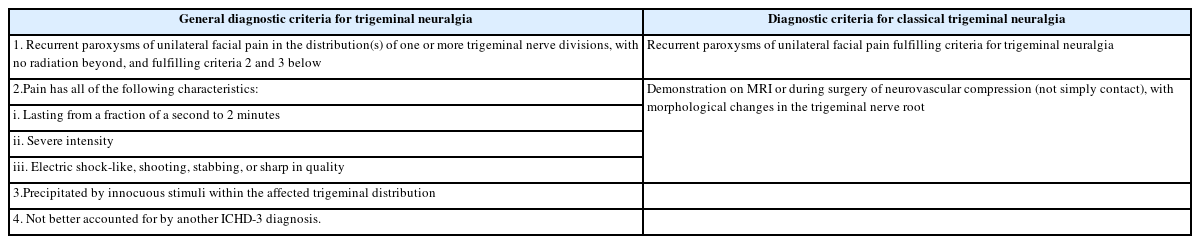
ICHD-3 diagnostic criteria for trigeminal neuralgia
COMPLICATIONS
Complications of TN and its treatment include neurotrophic keratitis, trigeminal trophic syndrome, and mental health conditions such as anxiety, depression, and social withdrawal.
Neurotrophic keratitis is a degenerative disorder characterized by reduced corneal sensitivity, spontaneous epithelial breakdown, and impaired corneal healing. Management is aimed at protecting the cornea and preventing vision loss.9
Trigeminal trophic syndrome is characterized by skin ulceration and dysesthesias, which are abnormal and unpleasant sensations that may be elicited by touch. The most common causes include ischemic medullary or pontine stroke and therapeutic ablation of the trigeminal nerve; additional causes include trauma, herpes zoster infection, and craniofacial surgery. Management is directed toward symptom control, promotion of wound healing, and prevention of skin infection.10
In addition, TN carries a substantial psychological burden, including anxiety, depression, and social withdrawal, underscoring the need for holistic patient care.11
DENTAL IMPLICATIONS
TN frequently mimics odontogenic pain because it may present primarily as tooth, jaw, or cheek pain, leading to misdiagnosis and unnecessary dental procedures. Unlike odontogenic pain, TN typically persists despite local anesthesia. Dentists and physicians should therefore recognize the dental implications of TN to distinguish it from dental disease and other orofacial pain conditions, ensure prompt referral, and facilitate timely interdisciplinary management when needed.12
Orofacial pain may compromise oral hygiene and thereby increase the risk of dental infection. In addition, sensory neuropathy resulting from iatrogenic injury to the terminal branches of the mandibular division of the trigeminal nerve in the infratemporal fossa may occur during dental anesthetic procedures, such as inferior alveolar nerve block or lingual nerve block. In contrast to odontogenic pain, TN-related pain typically persists or worsens after administration of dental anesthesia. A detailed history, physical examination, and appropriate imaging studies, including MRI, should be obtained, and the diagnosis of TN should be based on the five ICHD-3 clinical diagnostic criteria before referral to neurosurgery to reduce misdiagnosis and improve patient outcomes.13
THERAPEUTIC MANAGEMENT
Pharmacological therapy is the first-line treatment for TN. Carbamazepine and oxcarbazepine remain the first-line medications and have demonstrated efficacy in reducing attack frequency and severity. Alternative or adjunctive agents include gabapentin, lamotrigine, baclofen, and phenytoin, particularly in refractory cases or in patients with secondary TN.14
Botulinum toxin injections may represent an alternative for patients with TN, short-lasting unilateral neuralgiform headache attacks, or high-frequency episodic migraine, but only after a clear explanation has been provided, informed consent has been obtained, and other pharmacological therapies have failed or caused serious adverse effects. Greater occipital nerve blocks may be considered for cluster headache and occipital neuralgia, although these are not absolute indications. In some cases, steroids are administered concurrently for cluster headache. Compared with botulinum toxin injections, nerve blocks are less costly, may be administered more frequently depending on patient need, and require fewer injections.15
Lidocaine-medicated plaster (LMP) is an adjunctive therapy that has provided pain relief in some reported cases of TN, particularly in cases refractory to oral antiepileptic drugs. Two retrospective studies have suggested that LMP may be an effective and safe adjunctive option for selected patients with TN. In addition, a randomized, double-blind, parallel-group, vehicle-controlled PATCH trial of 5% LMP conducted at five study centers demonstrated a significant reduction in weekly mean pain severity and lower treatment failure rates than placebo.16
A randomized, double-blind, placebo-controlled proof-of-concept trial conducted in Denmark investigated the efficacy and safety of erenumab, a calcitonin gene-related peptide (CGRP) receptor monoclonal antibody, in patients with TN. Although erenumab was well tolerated, it did not significantly reduce pain compared with placebo, suggesting that it has no established therapeutic effect in the management of TN. These findings further suggest that CGRP, which plays a major role in migraine pathophysiology, may have little or no role in the pathophysiology of TN.17
Surgical intervention is considered when medical therapy is ineffective or poorly tolerated. MVD provides durable pain relief in appropriately selected patients. Less invasive options, including stereotactic radiosurgery and percutaneous ablative procedures, offer effective alternatives with lower perioperative risk. Minimally invasive procedures have increasingly supplemented, and in some settings replaced, more invasive techniques. Although stereotactic radiosurgery is a valuable treatment option, MVD remains the gold standard for classical TN with vascular compression. Radiosurgery is generally considered an alternative for high-risk patients because it is associated with shorter hospital stays, faster recovery, greater convenience as an outpatient procedure, and a lower postoperative complication risk. As a nerve-targeted intervention, it may also reduce recurrence rates. In addition, recent studies have explored basimglurant, a novel negative allosteric modulator of glutamate receptor 5 with therapeutic and metabotropic effects, in the management of TN. With a long half-life and favorable oral bioavailability, basimglurant has been reported to be relatively potent, safe, and selective in humans when administered once daily at the prescribed dose. However, because basimglurant remains under clinical investigation, it has not been approved as a first-line treatment for TN. Further studies are needed to establish its role in clinical practice.18
Furthermore, psychological support through effective health education, counseling, multidisciplinary care, appropriate patient selection for treatment, and adequate follow-up is essential for optimizing healthcare delivery and improving patient outcomes (Figure 1).19,20
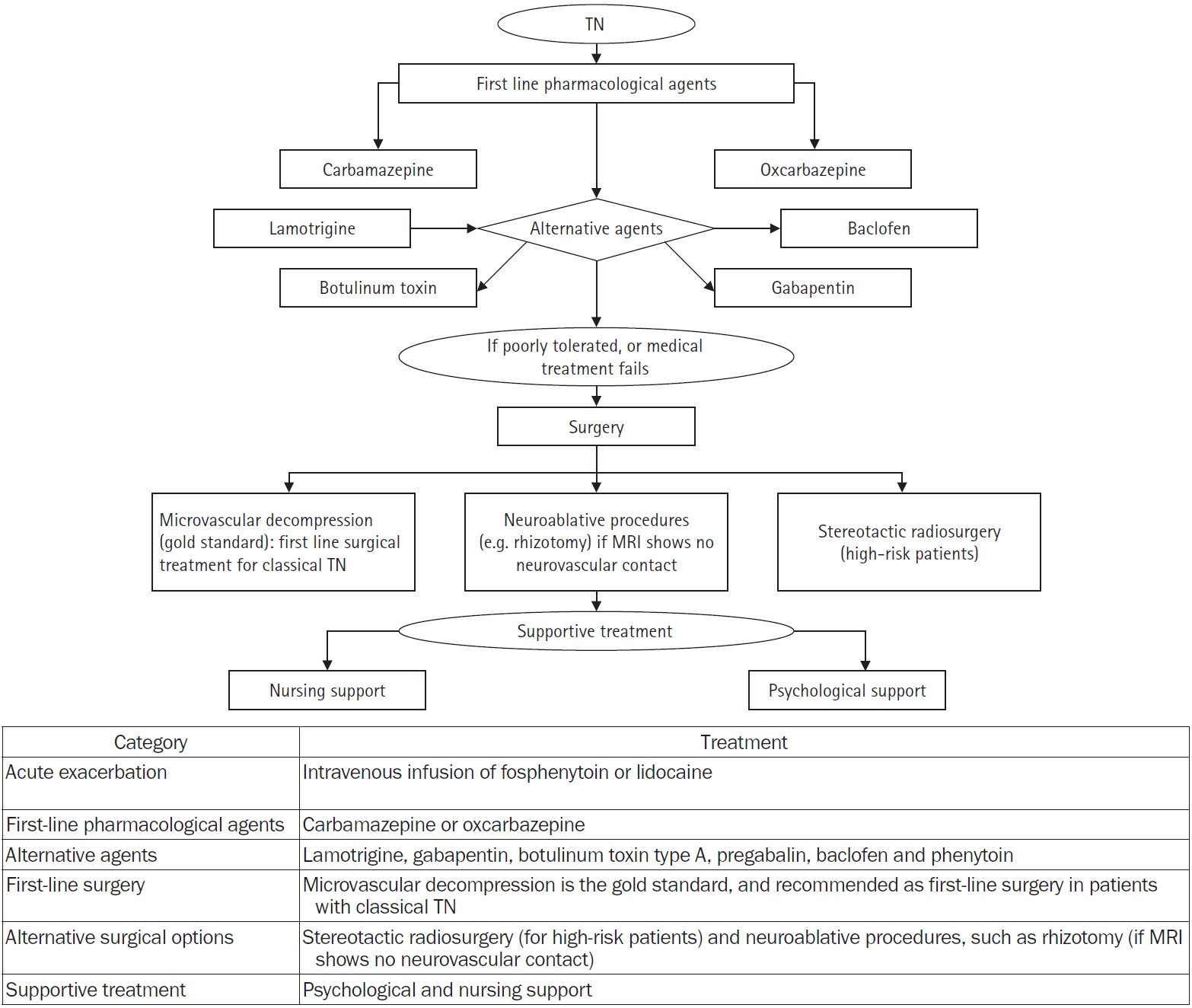
Treatment overview of TN.
TN, trigeminal neuralgia; MRI, magnetic resonance imaging.
IMPLICATIONS FOR HEADACHE AND PAIN RESEARCH
From the perspective of headache medicine, TN serves as a model disorder linking peripheral nerve pathology to central pain processing. Future research priorities include improved phenotyping of continuous pain components, identification of biomarkers that predict treatment response, and development of mechanism-based therapies targeting ion channel dysfunction and central sensitization.
FUTURE DIRECTIONS
Emerging therapies targeting novel molecular pathways, together with advances in neurosurgical techniques, hold promise for improving outcomes. Further research is needed to optimize patient selection, clarify mechanisms underlying continuous pain components, and develop disease-modifying interventions.
CONCLUSION
TN is a debilitating neuropathic pain disorder that requires prompt recognition and accurate diagnosis. Advances in understanding its pathophysiology and management have expanded therapeutic options and supported more individualized, multidisciplinary care. Improved awareness across medical and dental disciplines is essential to reduce misdiagnosis and improve patient quality of life.
Notes
AVAILABILITY OF DATA AND MATERIAL
Not applicable.
AUTHOR CONTRIBUTIONS
Conceptualization: EN; Resources: EN, CA, DA; Writing–original draft: EN, CA, DA; Writing–review & editing: EN, CA, DA.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported. This manuscript was prepared with the assistance of ChatGPT-4 (OpenAI), used on January 26, 2026, for grammar and language refinement. All content generated with AI assistance was independently verified by the authors.
FUNDING STATEMENT
None.
ACKNOWLEDGMENTS
None.