The Impact of Limited Insurance Coverage on Long-Term Persistence with Anti-CGRP Monoclonal Antibody Therapy: A Multicenter Real-World Study in Korea
Article information

Abstract
Purpose
Anti-calcitonin gene-related peptide monoclonal antibodies (anti-CGRP mAbs) are effective preventive therapies for migraine. However, their high cost limits long-term use. In Korea, coverage of anti-CGRP mAbs by the National Health Insurance Service (NHIS) is highly restricted. This study aimed to evaluate the association between NHIS coverage and treatment persistence in a real-world setting.
Methods
This retrospective multicenter study included adult patients with migraine (≥18 years) who received anti-CGRP mAb therapy at four tertiary hospitals in Korea. Treatment compliance was assessed using persistence, defined as continuous treatment duration; persistence rates; and adherence, defined as the proportion of days covered. Reasons for treatment discontinuation were also analyzed. Treatment compliance was compared according to NHIS coverage, and treatment effectiveness was compared according to NHIS coverage and treatment continuation.
Results
Among 140 patients treated with anti-CGRP mAbs, only 12 (8.6%) received NHIS-covered therapy. Compared with the non-covered group, the NHIS-covered group had a lower discontinuation rate (50.0% [6/12] vs. 73.4% [94/128]; p=0.101) and higher persistence rates at 6 months (80.0% vs. 66.0%; p=0.493) and 12 months (66.7% vs. 47.2%; p=0.312). However, these differences were not statistically significant. Treatment effectiveness, assessed by changes in monthly headache days, did not differ significantly according to NHIS coverage or treatment continuation.
Conclusion
Treatment persistence appears to be influenced by multiple factors in real-world practice. NHIS coverage may support treatment continuation by improving access and reducing the financial burden. These findings highlight the importance of healthcare-system factors in optimizing long-term preventive treatment strategies for migraine.
INTRODUCTION
Migraine is a common and debilitating neurological disorder. Globally, migraines impose a significant burden on individuals and healthcare systems, leading to decreased productivity and reduced quality of life.1,2 Effective management is crucial for patients with migraines to minimize this burden.
Anti-calcitonin gene-related peptide monoclonal antibodies (anti-CGRP mAbs) have emerged as a promising treatment option for migraine prevention.3 Treatments such as erenumab, galcanezumab, fremanezumab, and eptinezumab target CGRP or its receptor, thereby interrupting the pathophysiological mechanisms of migraine.4 Clinical trials have demonstrated that these medications effectively reduce migraine frequency and improve patient-reported outcomes, making them an attractive option for patients unresponsive to traditional therapies.5
Despite the proven efficacy of anti-CGRP mAbs, compliance including persistence and adherence remains significant challenges in real-world clinical settings.6 Compliance is important to achieve effectiveness with anti-CGRP mAbs.7 Anti-CGRP mAbs are considerably more expensive than conventional migraine preventive treatments.8 The impact of National Health Insurance Service (NHIS) coverage on real-world treatment compliance is not well understood. In countries like South Korea, where the NHIS offers limited coverage for migraine,9 it is important to explore how reimbursement policies affect patient behavior. While some studies have mentioned economic barriers,6 few have examined this issue in detail using real-world data within NHIS systems.
This study aims to analyze the proportion of patients receiving NHIS coverage and to compare treatment compliance between those receiving anti-CGRP mAbs with NHIS-covered and non-covered. By examining the impact of coverage status on treatment continuation, the study aims to provide insights for optimizing healthcare policy and enhancing the long-term management of migraine.
MATERIALS AND METHODS
1. Study design and participants
This retrospective, multicenter observational study was conducted at four centers (two tertiary referral university hospitals, one secondary referral university hospital, one general hospital) and approved by the Institutional Review Board of Dongtan Hallym University Sacred Heart Hospital, Republic of Korea (approval number: HDT 2024-08-010-001). The study adhered to the ethical principles outlined in the Declaration of Helsinki.
The inclusion criteria specified adult patients aged 18 years or older with a confirmed diagnosis of migraine, based on the International Classification of Headache Disorders, 3rd edition,10 who received anti-CGRP mAbs therapy between July 2022 and June 2023.
2. Data collection
Patient demographics, including age, sex distribution, body mass index, migraine subtypes (such as migraine with or without aura, chronic migraine, pure menstrual migraine, and menstrual-related migraine), baseline headache characteristics including monthly headache days (MHD), monthly medication days and severity were collected. Age at migraine onset and disease duration before anti-CGRP mAbs therapy initiation were also collected. Patients completed a questionnaires including Headache Impact Test-6 (HIT-6), Patient Health Questionnaire-9 (PHQ-9), Generalized Anxiety Disorder-7 (GAD-7). Data on anti-CGRP mAbs type (galcanezumab or fremanezumab), number of injections, and injection intervals were also collected. In addition, these factors were compared between patients with and without NHIS coverage.
3. Compliance analysis
Participants who received their first anti-CGRP mAbs injection between July 2022 and June 2023 were monitored for up to 1 year. Treatment compliance was evaluated using two complementary measures: persistence and adherence.
Persistence was defined as the duration of continuous treatment with anti-CGRP mAbs, representing treatment continuation over time. Discontinuation was defined as cessation of treatment during the follow-up period. A maximum interval of 60 days between doses, referred to as the “60-day allowable gap,” was permitted. The persistence rate, representing the percentage of patients who remained on treatment at specific time points, was calculated at 6 and 12 months.
Adherence was assessed using the Proportion of Days Covered (PDC) method, a widely recognized approach in retrospective studies for evaluating medication adherence.11,12 PDC was calculated as the ratio of the total number of days the medication was available to the patient to the total number of days in the follow-up period. Each injection of anti-CGRP mAbs was considered to provide 30 days of coverage for monthly regimens and 90 days for quarterly regimens, starting from the prescription date. Patients with a PDC of ≥80% were classified as adherent, as this threshold is widely accepted as an indicator of good medication adherence in adherence studies.
To examine the impact of coverage status, participants were categorized into two groups: those with and without NHIS coverage. Persistence, persistence rates, and adherence were compared between the groups. Reasons for treatment discontinuation were also analyzed.
4. Assessment of treatment response
Treatment response was evaluated in terms of both effectiveness and safety. Treatment effectiveness was assessed using MHD at baseline and during follow-up visits (1, 3, 6, and 12 months). To evaluate the potential relationship between treatment effectiveness and treatment discontinuation, MHD during follow-up were compared according to insurance coverage and treatment discontinuation. Safety was assessed by analyzing adverse events reported during treatment.
5. Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics 29.0.2.0 (IBM Corp.). Descriptive statistics included demographic data and baseline disease characteristics. Continuous data are presented as mean and standard deviation or median and interquartile range (IQR), and categorical data are presented as frequencies and percentages. Group comparisons for categorical variables were conducted using the chi-square test. Fisher’s exact test was used for categorical comparisons when the sample size in some categories was small and did not meet the assumptions required for the chi-square test. For continuous variables that were not normally distributed, the Mann-Whitney U-test was applied. Statistical significance was set at a p-value of less than 0.05. Missing data were handled using an available-case analysis approach. Analyses were performed using all available observations for each outcome variable. Due to the retrospective nature of the study, follow-up data was not available for all patients at each time point.
RESULTS
1. Patient demographics
A total of 140 patients were enrolled in the study, of whom 12 (8.6%) received anti-CGRP mAbs therapy covered by NHIS. A comparison was made between patients who received NHIS-covered treatment and those who did not, with detailed results presented in Table 1. Patients in the NHIS-covered group had a significantly higher number of MHD compared to those without coverage (25.5 [IQR, 14.0–28.0] vs. 15.0 [IQR, 10.0–20.0], p=0.027). No significant differences were observed between the two groups in terms of age, age of onset, sex distribution, migraine subtype, disease duration before anti-CGRP mAbs therapy (Table 1).

Comparison of clinical characteristics and treatment by insurance coverage status for anti-CGRP mAb therapy (n=140)
2. Compliance analysis
The treatment discontinuation rate was lower in the NHIS-covered group compared to the non-covered group (50.0% [6/12] vs. 73.4% [94/128], p=0.101) (Table 2). The distribution of the total number of injections is shown in Figure 1. Compared to NHIS-covered group, non-covered group had a relatively higher proportion of those receiving fewer than six injections (Figure 1). Among patients who discontinued treatment in the NHIS-covered group, lack of effectiveness was the most common reason (4/6, 66.7%), followed by headache improvement (2/6, 33.3%). In the non-covered group, discontinuation occurred for various reasons, including headache improvement (30/94, 31.9%), loss to follow-up (33/94, 35.1%), lack of effectiveness (17/94, 18.1%), adverse events (7/94, 7.4%), financial reasons (3/94, 3.2%), and other reasons (4/94, 4.3%) (Table 2).

Comparison of treatment according to NHIS coverage
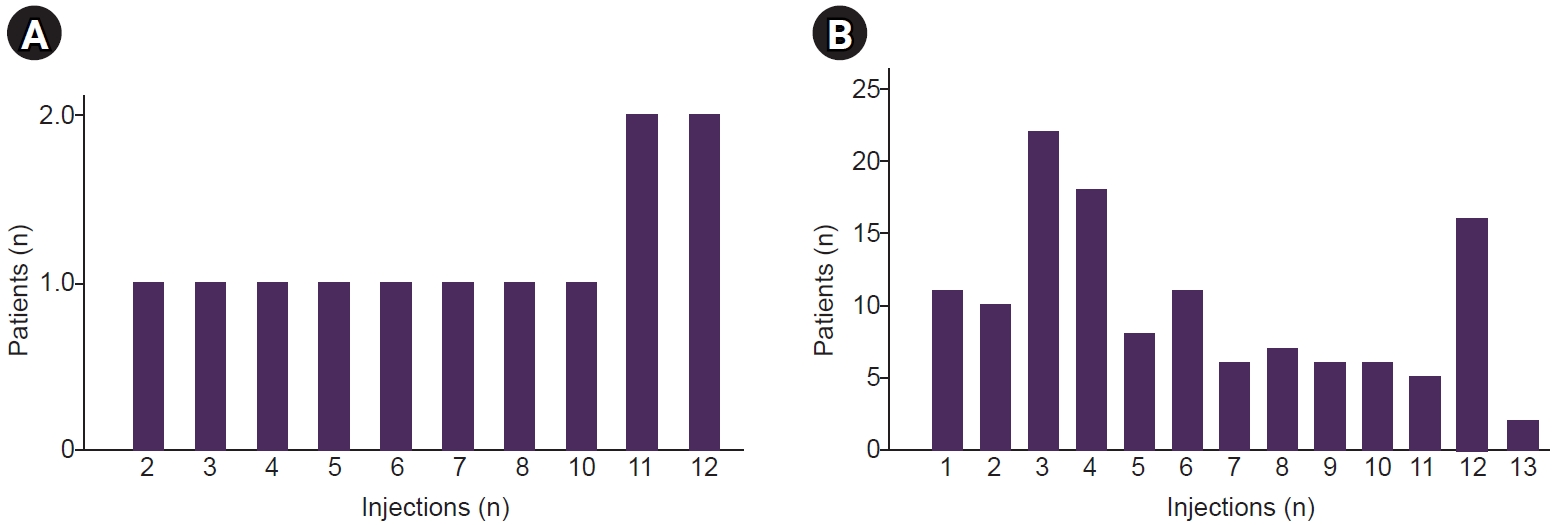
Distribution of the number of injections by insurance coverage (National Health Insurance Service [NHIS]-covered vs. non-covered). (A) NHIS-covered patients. (B) Non-covered patients.
At 6 months, 83.8% (10/12) of patients in the NHIS-covered group and 78.1% (100/128) in the non-covered group remained in follow-up. Among them, the persistence rate was higher in the NHIS-covered group (80.0% [8/10]) than in the non-covered group (66.0% [66/100], p=0.493). At 12 months, 75.0% (9/12) of patients in the NHIS-covered group and 56.2% (72/128) in the non-covered group remained in follow-up. Among them, the persistence rate remained higher in the NHIS-covered group (66.7% [6/9]) than in the non-covered group (47.2% [34/72]), though the difference was not statistically significant (p=0.312) (Table 2).
The median duration of treatment (days, IQR) was longer in the NHIS-covered group (313.0 [120.3–374.0]) compared to the non-covered group (177.0 [91.3–358.7]) (p=0.214). The total number of injections (median, IQR) was slightly higher in the NHIS-covered group (7.5 [4.3–11.0]) than in the non-covered group (5.0 [3.0–9.0]) (p=0.140). The days of coverage (IQR) were greater in the NHIS-covered group (225 [127.5–330.0]) compared to the non-covered group (150 [90–270]) (p=0.140). The adherence (% IQR) was slightly higher in the NHIS-covered group (86.7 [57.5–100]) than in the non-covered group (79.9 [43.3–100]) (p=0.300). The proportion of adherent patients (n, %) was higher in the NHIS-covered group (66.7% [8/12]) than in the non-covered group (50.0% [64/128]) (p=0.369). However, none of these differences were statistically significant (Table 2).
3. Assessment of treatment response
Treatment effectiveness according to insurance coverage showed that patients in the NHIS-covered group had significantly higher baseline MHD compared with those in the non-covered group (21.7±8.0 vs. 15.7±8.3, p=0.026). MHD during early follow-up visits were also higher in the NHIS-covered group (16.4±10.6 vs. 9.1±9.1 at 1 month, p=0.005; 15.3±10.4 vs. 8.1±8.0 at 3 months, p=0.012). However, differences at 6 and 12 months were not statistically significant (14.6±10.6 vs. 7.5±6.9 at 6 months, p=0.071; 10.9±10.4 vs. 7.8±7.4 at 12 months, p=0.407). Despite these differences in absolute MHD values, the magnitude of improvement from baseline did not differ significantly between the two groups at any time point (Table 3).

Change in MHD according to insurance coverage and treatment discontinuation
Treatment effectiveness was also analyzed according to treatment discontinuation. Baseline MHD were similar between patients who continued treatment and those who discontinued therapy (15.6±6.8 vs. 16.5±8.9, p=0.709). During follow-up, MHD consistently tended to be lower in patients who continued treatment compared with those who discontinued therapy; however, these differences did not reach statistical significance at any time point. At 12 months, patients who continued treatment showed numerically lower MHD compared with those who discontinued (6.7±5.3 vs. 10.0±9.9, p=0.469). Similarly, reduction in MHD from baseline were comparable between the continued and discontinued groups throughout follow-up (Table 3).
Adverse events were reported in 19 patients (13.6%) overall, including two patients (16.7%, 2/12) in the NHIS-covered group and 17 patients (13.3%, 17/128) in the non-covered group (p=0.667). Discontinuation due to adverse events was reported in the non-covered group. These adverse events led to treatment discontinuation were reported in seven patients, including allergic reactions (n=3), constipation (n=1), weight gain (n=1), vomiting (n=1), and abnormal uterine bleeding (n=1). No serious adverse events were reported (Table 2).
DISCUSSION
This study examined the proportion of patients receiving NHIS coverage and its association with treatment compliance. Only a small proportion of patients were covered by NHIS. The NHIS-covered group had a lower discontinuation rate, whereas a larger proportion of non-covered patients discontinued treatment within the first six injections. Treatment persistence rates at 6 and 12 months were numerically higher in the NHIS-covered group; however, these differences were not statistically significant. Importantly, treatment effectiveness, as measured by changes in MHD, did not differ significantly according to NHIS coverage or treatment continuation during follow-up.
Despite the growing evidence supporting the efficacy of anti-CGRP mAbs,13-15 only a small proportion of patients in this study received NHIS coverage. This limited access likely reflects the relatively strict reimbursement criteria of the current NHIS, which may hinder treatment initiation or continuation despite clinical need. The low proportion of NHIS-covered patients highlights the need for better alignment between clinical needs and institutional support. Notably, HIT-6 scores did not differ significantly between the NHIS-covered and non-covered groups (60.9±7.9 vs. 61.4±7.8, p=0.654) (Table 1), indicating comparable levels of migraine-related disability. These findings suggest that the current NHIS coverage criteria may not fully reflect the real-world disability or patient-reported disease burden in migraine.
The NHIS-covered group showed a lower discontinuation rate over 12 months, whereas a higher proportion of patients in the non-covered group discontinued treatment within the first 6 months. Persistence rates at both 6 and 12 months were numerically higher in the NHIS-covered group; however, these differences did not reach statistical significance, possibly due to the small sample size. These findings may suggest that insurance coverage contributes to treatment continuation, particularly during the early phase of therapy.
However, treatment continuation is likely influenced by multiple factors beyond insurance status alone. Previous studies have reported that higher headache frequency is associated with lower persistence, often driven by inadequate perceived efficacy and unmet treatment expectations.16 Beyond the initial treatment period, factors such as perceived efficacy, tolerability, and overall disease burden may further influence patients’ decisions to continue therapy.17 Indeed, lack of perceived efficacy has been consistently reported as one of the most common reasons for discontinuation among patients treated with anti-CGRP mAbs.6,17-19 In the present study, lack of effectiveness was also a common reason for discontinuation.
Despite the lack of significant differences in treatment effectiveness between groups, both NHIS-covered and non-covered patients showed reductions in MHD during follow-up, indicating that anti-CGRP mAbs were clinically effective in real-world practice. However, the magnitude of improvement was comparable between groups, and no significant differences were observed in the reduction in MHD from baseline according to insurance coverage or whether treatment was continued. Notably, despite having higher baseline MHD and consistently higher MHD during follow-up, patients in the NHIS-covered group showed numerically higher persistence rates compared with the non-covered group. This pattern suggests that the higher persistence rate observed in the NHIS-covered group cannot be fully explained by differences in treatment effectiveness.
Taken together, these findings suggest that treatment continuation was not solely explained by differences in treatment effectiveness. Instead, the numerically higher persistence observed in the NHIS-covered group indicates that insurance coverage may facilitate treatment continuation independent of clinical response, likely by reducing financial barriers and improving access to therapy. In addition, factors such as perceived efficacy, tolerability, overall disease burden, and patient expectations may further influence patients’ decisions to continue treatment in real-world practice.
Sustained treatment persistence may be particularly important in the context of anti-CGRP mAbs therapy, as some patients demonstrate delayed or late treatment responses that may not be apparent during the early treatment period.20 Several real-world studies have reported continued improvements in headache frequency, disability, and quality of life beyond the initial treatment phase.21,22 In line with these findings, our results also showed a consistent trend toward greater reductions in MHD among patients who continued treatment compared with those who discontinued, although these differences did not reach statistical significance.
Early treatment discontinuation may limit the opportunity to achieve the full therapeutic and functional benefits of preventive treatment. From an economic perspective, early discontinuation may also reduce cost-effectiveness by limiting potential long-term benefits, including reduced healthcare utilization, improved productivity, and decreased disability.23 Therefore, factors that support sustained treatment may play an important role in optimizing both clinical and economic outcomes in routine practice.
Several limitations should be considered. First, the small sample size of the NHIS-covered group (n=12) may have limited the statistical power to detect significant effects. Therefore, the findings should be interpreted with caution, and larger studies are needed to confirm these results. Second, although this study evaluated treatment discontinuation and included reasons for discontinuation, treatment decisions in real-world practice are influenced by multiple factors that were not fully captured. These include patient expectations, perceived effectiveness, psychological factors (e.g., anxiety and depression), and interactions with healthcare providers. Third, due to the retrospective design, for patients who were lost to follow-up, the reasons for treatment discontinuation may not have been fully captured, which could have introduced bias. Fourth, although treatment effectiveness was assessed using reduction in MHD, other clinically relevant outcomes— such as quality of life, functional disability, and ≥50% responder rates—were not evaluated. In addition, factors related to healthcare access—such as private insurance coverage, out-of-pocket costs, and availability of follow-up care—may have influenced treatment continuation but were not assessed.
CONCLUSION
In this real-world study, only a small proportion of migraine patients receiving anti-CGRP mAbs therapy were covered by the NHIS. Treatment persistence may be influenced by multiple factors beyond clinical response, including non-clinical factors such as access to therapy and financial burden. These findings highlight the potential importance of healthcare system factors, such as NHIS coverage, in supporting sustained preventive treatment in routine clinical practice.
Notes
AVAILABILITY OF DATA AND MATERIAL
The data presented in this study are available upon reasonable request from the corresponding author.
AUTHOR CONTRIBUTIONS
Conceptualization: MKK, SJC; Data curation: MKK; Formal analysis: MKK; Funding acquisition: MKK, MJC; Investigation: MKK, JHS, MJC, YHK, YH, HJI, SJC; Methodology: MKK, JHS, MJC, YHK, YH, HJI, SJC; Supervision: SJC; Writing–original draft: MKK; Writing–review & editing: MKK, JHS, MJC, YHK, YH, HJI, SJC.
CONFLICT OF INTEREST
Soo-Jin Cho is the Editor-in-Chief of Headache and Pain Research and was not involved in the review process of this article. All authors have no other conflicts of interest to declare.
FUNDING STATEMENT
This research was supported by the 2024 headache research grant from the Korean Headache Society.
ACKNOWLEDGMENTS
None.