
Articles
- Page Path
- HOME > Headache Pain Res > Volume 27(2); 2026 > Article
-
Original Article
The Impact of Limited Insurance Coverage on Long-Term Persistence with Anti-CGRP Monoclonal Antibody Therapy: A Multicenter Real-World Study in Korea -
Mi-Kyoung Kang1
 , Jong-Hee Sohn2, Myoung-Jin Cha3, Yoo Hwan Kim4, Yooha Hong1, Hee-Jin Im1, Soo-Jin Cho1
, Jong-Hee Sohn2, Myoung-Jin Cha3, Yoo Hwan Kim4, Yooha Hong1, Hee-Jin Im1, Soo-Jin Cho1 -
Headache and Pain Research 2026;27(2):145-153.
DOI: https://doi.org/10.62087/hpr.2026.0007
Published online: June 4, 2026
1Department of Neurology, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwaseong, Republic of Korea
2Department of Neurology, Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Chuncheon, Republic of Korea
3Department of Neurology, National Police Hospital, Seoul, Republic of Korea
4Department of Neurology, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Republic of Korea
- Correspondence: Soo-Jin Cho, M.D., Ph.D. Department of Neurology, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, 7 Keunjaebong-gil, Hwaseong 18450, Republic of Korea Tel: +82-31-8086-2310, Fax: +82-31-8086-2317, E-mail: dowonc@naver.com
© 2026 The Korean Headache Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 619 Views
- 14 Download
Abstract
-
Purpose
- Anti-calcitonin gene-related peptide monoclonal antibodies (anti-CGRP mAbs) are effective preventive therapies for migraine. However, their high cost limits long-term use. In Korea, coverage of anti-CGRP mAbs by the National Health Insurance Service (NHIS) is highly restricted. This study aimed to evaluate the association between NHIS coverage and treatment persistence in a real-world setting.
-
Methods
- This retrospective multicenter study included adult patients with migraine (≥18 years) who received anti-CGRP mAb therapy at four tertiary hospitals in Korea. Treatment compliance was assessed using persistence, defined as continuous treatment duration; persistence rates; and adherence, defined as the proportion of days covered. Reasons for treatment discontinuation were also analyzed. Treatment compliance was compared according to NHIS coverage, and treatment effectiveness was compared according to NHIS coverage and treatment continuation.
-
Results
- Among 140 patients treated with anti-CGRP mAbs, only 12 (8.6%) received NHIS-covered therapy. Compared with the non-covered group, the NHIS-covered group had a lower discontinuation rate (50.0% [6/12] vs. 73.4% [94/128]; p=0.101) and higher persistence rates at 6 months (80.0% vs. 66.0%; p=0.493) and 12 months (66.7% vs. 47.2%; p=0.312). However, these differences were not statistically significant. Treatment effectiveness, assessed by changes in monthly headache days, did not differ significantly according to NHIS coverage or treatment continuation.
-
Conclusion
- Treatment persistence appears to be influenced by multiple factors in real-world practice. NHIS coverage may support treatment continuation by improving access and reducing the financial burden. These findings highlight the importance of healthcare-system factors in optimizing long-term preventive treatment strategies for migraine.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
CONCLUSION
AVAILABILITY OF DATA AND MATERIAL
The data presented in this study are available upon reasonable request from the corresponding author.
AUTHOR CONTRIBUTIONS
Conceptualization: MKK, SJC; Data curation: MKK; Formal analysis: MKK; Funding acquisition: MKK, MJC; Investigation: MKK, JHS, MJC, YHK, YH, HJI, SJC; Methodology: MKK, JHS, MJC, YHK, YH, HJI, SJC; Supervision: SJC; Writing–original draft: MKK; Writing–review & editing: MKK, JHS, MJC, YHK, YH, HJI, SJC.
CONFLICT OF INTEREST
Soo-Jin Cho is the Editor-in-Chief of Headache and Pain Research and was not involved in the review process of this article. All authors have no other conflicts of interest to declare.
FUNDING STATEMENT
This research was supported by the 2024 headache research grant from the Korean Headache Society.
ACKNOWLEDGMENTS
None.
| NHIS-covered (n=12) | Non-covered (n=128) | p-value | |
|---|---|---|---|
| Age (yr) | 43.6±15.7 | 44.7±11.8 | 0.902 |
| Sex, female | 10 (83.3) | 106 (82.8) | 0.662 |
| BMI (kg/m2) | 22.7±4.2 | 22.2±3.3 | 0.783 |
| Hypertension | 4 (33.3) | 13 (10.2) | 0.060 |
| DM | 0 | 3 (2.3) | 0.637 |
| Migraine subtype | |||
| Chronic migraine | 11 (91.7) | 80 (62.5) | 0.057 |
| Episodic migraine | 1 (8.3) | 48 (37.5) | |
| Without aura | 11 (91.7) | 120 (93.8) | 0.565 |
| With aura | 1 (8.3) | 8 (6.3) | |
| PMM | 0 | 7/123 (5.7) | 0.540 |
| MRM | 0 | 12/123 (9.8)* | |
| Baseline headache characteristics | |||
| Monthly headache days | 25.5 (14.0–28.0) | 15.0 (10.0–20.0) | 0.027 |
| Monthly medication days | 13.0 (3.0–25.0) | 10.0 (6.0–20.0) | 0.856 |
| Monthly headache days more than 26 | 6 (50.0) | 23 (18.0) | 0.018 |
| Age of onset (yr) | 20.9±10.3 | 27.1±12.7 | 0.152 |
| Disease duration before CGRP (yr) | 19.2±20.0 | 15.9±11.2 | 0.876 |
| Questionnaires | |||
| HIT-6 | 60.9±7.9 | 61.4±7.8 | 0.654 |
| GAD-7 | 5.5 (2.8‒9.8) | 5.0 (2.0‒8.8) | 0.436 |
| PHQ-9 | 8.5 (5.0‒13.3) | 7.0 (4.0‒9.0) | 0.150 |
| Anti-CGRP mAb type | |||
| Galcanezumab | 6 (50.0) | 53 (41.4) | 0.792 |
| Fremanezumab | 6 (50.0) | 75 (58.6) | |
| Prior anti-CGRP mAb treatment | 3 (25.0) | 23 (18.0) | 0.391 |
Values are presented as mean±standard deviation, number (%), or median (interquartile range).
anti-CGRP mAb, anti-calcitonin gene-related peptide monoclonal antibody; NHIS, National Health Insurance Service; BMI, body mass index; DM, diabetes mellitus; PMM, pure menstrual migraine; MRM, menstrual-related migraine; CGRP, calcitonin gene-related peptide; HIT-6, Headache Impact Test-6; GAD-7, Generalized Anxiety Disorder 7-Item Scale; PHQ-9, Patient Health Questionnaire-9.
*PMM and MRM analyses were performed in 123 patients in the non-covered group because data were unavailable for 5 patients.
| NHIS-covered (n=12) | Non-covered (n=128) | p-value | |
|---|---|---|---|
| Total number of injections | 7.5 (4.3‒11.0) | 5.0 (3.0‒9.0) | 0.140 |
| Interval between injections (day) | 32.1 (30.7‒33.9) | 31.9 (30.0‒36.0) | 0.867 |
| Anti-CGRP mAb discontinuation | 6 (50.0) | 94 (73.4) | 0.101 |
| Reasons for discontinuation | |||
| Lack of effectiveness | 4/6 (66.7) | 17/94 (18.1) | |
| Headache improvement | 2/6 (33.3) | 30/94 (31.9) | |
| Loss of follow-up | - | 33/94 (35.1) | |
| Adverse events* | - | 7/94 (7.4) | |
| Financial reasons | - | 3/94 (3.2) | |
| Others | - | 4/94 (4.3) | |
| Overall adverse events | 2/12 (16.7) | 17/128 (13.3) | 0.667 |
| Adherence | 86.7 (57.5‒100) | 79.9 (43.3‒100) | 0.300 |
| Days covered | 225 (127.5‒330.0) | 150 (90.0‒270.0) | 0.140 |
| Adherent | 8 (66.7) | 64 (50.0) | 0.369 |
| Persistence | |||
| Duration of treatment (day) | 313.0 (120.3‒374.0) | 177.0 (91.3‒358.7) | 0.214 |
| At 6 months | |||
| Follow-up | 10 (83.8) | 100 (78.1) | >0.99 |
| Persistence rate | 8/10 (80.0) | 66/100 (66.0) | 0.493 |
| At 12 months | |||
| Follow-up | 9 (75.0) | 72 (56.2) | 0.240 |
| Persistence rate | 6/9 (66.7) | 34/72 (47.2) | 0.312 |
Values are presented as median (interquartile range) or number (%).
NHIS, National Health Insurance Service; Anti-CGRP mAb, anti-calcitonin gene-related peptide monoclonal antibody.
*Including allergic reactions (n=3), constipation (n=1), weight gain (n=1), vomiting (n=1), and abnormal uterine bleeding (n=1).
| Variable | MHD, mean±SD | ||||
|---|---|---|---|---|---|
| Baseline | After 1 month | After 3 months | After 6 months | After 12 months | |
| NHIS coverage | |||||
| Covered (n=12) | 21.7±8.0 | 16.4±10.6 | 15.3±10.4 | 14.6±10.6 | 10.9±10.4 |
| Non-covered (n=128) | 15.7±8.3 | 9.1±9.1 | 8.1±8.0 | 7.5±6.9 | 7.8±7.4 |
| p-value | 0.026 | 0.005 | 0.012 | 0.071 | 0.407 |
| Reduction in MHD from baseline | |||||
| Covered | 5.3±7.5 | 6.3±9.8 | 5.3±12.6 | 10.6±10.1 | |
| Non-covered | 6.0±7.5 | 6.8±7.8 | 7.6±7.3 | 7.7±9.0 | |
| p-value* | 0.398 | 0.631 | 0.523 | 0.6 | |
| Treatment discontinuation | |||||
| Continued (n=40) | 15.6±6.8 | 8.2±7.7 | 8.9±7.9 | 8.4±6.9 | 6.7±5.3 |
| Discontinued (n=100) | 16.5±8.9 | 10.9±10.3 | 9.1±9.1 | 8.1±8.1 | 10.0±9.9 |
| p-value | 0.709 | 0.253 | 0.732 | 0.381 | 0.469 |
| Reduction in MHD from baseline | |||||
| Continued | 6.9±6.7 | 6.9±7.3 | 7.1±8.1 | 8.9±7.4 | |
| Discontinued | 5.4±8.3 | 6.3±8.5 | 7.6±7.9 | 7.0±10.8 | |
| p-value* | 0.255 | 0.724 | 0.925 | 0.291 | |
- 1. Dong L, Dong W, Jin Y, Jiang Y, Li Z, Yu D. The Global burden of migraine: a 30-year trend review and future projections by age, sex, country, and region. Pain Ther 2025;14:297-315.ArticlePubMedPMCPDF
- 2. Leonardi M, Raggi A. A narrative review on the burden of migraine: when the burden is the impact on people's life. J Headache Pain 2019;20:41.ArticlePubMedPMCPDF
- 3. Kim BS, Chung PW, Chung JM, et al. Evidence-based recommendations on pharmacologic treatment for migraine prevention: a clinical practice guideline from the Korean Headache Society. Headache Pain Res 2025;26:5-20.ArticlePDF
- 4. Romozzi M, Munafò A, Burgalassi A, et al. Pharmacological differences and switching among anti-CGRP monoclonal antibodies: a narrative review. Headache 2025;65:342-352.ArticlePubMed
- 5. Oliveira R, Gil-Gouveia R, Puledda F. CGRP-targeted medication in chronic migraine - systematic review. J Headache Pain 2024;25:51.ArticlePubMedPMCPDF
- 6. Kang MK, Sohn JH, Cha MJ, et al. One-year compliance after calcitonin gene-related peptide monoclonal antibody therapy for migraine patients in a real-world setting: a multicenter cross-sectional study. J Clin Med 2025;14:734.ArticlePubMedPMC
- 7. Ray R, Virk GS, Regmi N, et al. Patient adherence and long-term tolerability of anti-calcitonin gene-related peptide (CGRP) monoclonal antibodies in migraine prevention: a systematic review. Cureus 2025;17:e91347.ArticlePubMedPMC
- 8. Nguyen JL, Munshi K, Peasah SK, et al. Trends in utilization and costs of migraine medications, 2017-2020. J Headache Pain 2022;23:111.ArticlePubMedPMCPDF
- 9. Health Insurance Review and Assessment Service. Detailed reimbursement criteria for anti-calcitonin gene-related peptide monoclonal antibodies [Internet]. Health Insurance Review and Assessment Service; 2024 [updated 2024; cited 2026 Jan 27]. Available from: https://www.hira.or.kr/bbsDummy.do?pgmid=HIRAA020002000100&brdScnBltNo=4&brdBltNo=10980#none
- 10. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018;38:1-211.ArticlePubMedPMCPDF
- 11. Lee WK, Lee J. Evaluation and improvement of adherence to medication. J Korean Med Assoc 2021;64:130-136.ArticlePDF
- 12. Prieto-Merino D, Mulick A, Armstrong C, et al. Estimating proportion of days covered (PDC) using real-world online medicine suppliers’ datasets. J Pharm Policy Pract 2021;14:113.ArticlePubMedPMCPDF
- 13. Muddam MR, Obajeun OA, Abaza A, et al. Efficacy and safety of anti-calcitonin gene-related peptide (CGRP) monoclonal antibodies in preventing migraines: a systematic review. Cureus 2023;15:e45560.ArticlePubMedPMC
- 14. Soni P, Chawla E. Efficacy and safety of anti-calcitonin gene-related peptide monoclonal antibodies for treatment of chronic migraine: a systematic review and network meta-analysis. Clin Neurol Neurosurg 2021;209:106893.ArticlePubMed
- 15. Iannone LF, Fattori D, Benemei S, Chiarugi A, Geppetti P, De Cesaris F. Long-term effectiveness of three anti-CGRP monoclonal antibodies in resistant chronic migraine patients based on the MIDAS score. CNS Drugs 2022;36:191-202.ArticlePubMedPMCPDF
- 16. Yuan D, Zhang Y, Li Q, et al. Factors affecting preventive treatment outcomes for patients with newly diagnosed chronic migraine and their compliance with treatment recommendations in Chongqing province, China: an open-label prospective study with retrospective baseline. Front Neurol 2020;11:227.ArticlePubMedPMC
- 17. Burgalassi A, Romozzi M, Vigani G, et al. Outcomes, unmet needs, and challenges in the management of patients who withdraw from anti-CGRP monoclonal antibodies: a prospective cohort study. Cephalalgia 2024;44:3331024241273968.ArticlePubMedPDF
- 18. de Dios A, Pagès-Puigdemont N, Ojeda S, et al. Persistence, effectiveness, and tolerability of anti-calcitonin gene-related peptide monoclonal antibodies in patients with chronic migraine. Headache 2025;65:24-34.ArticlePubMed
- 19. Barbanti P, Aurilia C, Torelli P, et al. Three-year treatment with anti-CGRP monoclonal antibodies modifies migraine course: the prospective, multicenter I-GRAINE study. J Neurol 2025;272:170.ArticlePubMedPMCPDF
- 20. Barbanti P, Aurilia C, Egeo G, et al. Late response to anti-CGRP monoclonal antibodies in migraine: a multicenter prospective observational study. Neurology 2023;101:482-488.ArticlePubMedPMC
- 21. Fernández-Bravo-Rodrigo J, Pascual-Morena C, Saz-Lara A, et al. Real-world effectiveness and safety of galcanezumab for the treatment of migraine: a systematic review and meta-analysis. Headache 2026;66:262-277.ArticlePubMedPMCPDF
- 22. Orlando B, Egeo G, Aurilia C, Fiorentini G, Barbanti P. Calcitonin gene-related peptide monoclonal antibodies: key lessons from real-world evidence. Brain Sci 2024;14:948.ArticlePubMedPMC
- 23. Lazaro-Hernandez C, Caronna E, Rosell-Mirmi J, et al. Early and annual projected savings from anti-CGRP monoclonal antibodies in migraine prevention: a cost-benefit analysis in the working-age population. J Headache Pain 2024;25:21.ArticlePubMedPMCPDF
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-
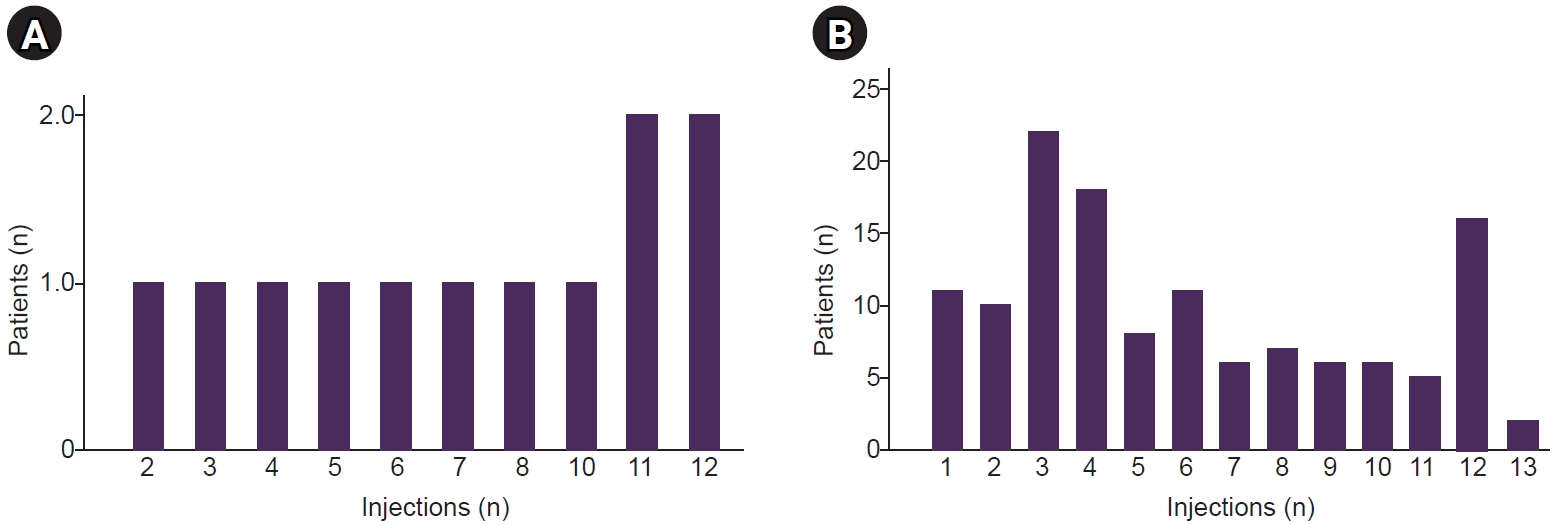
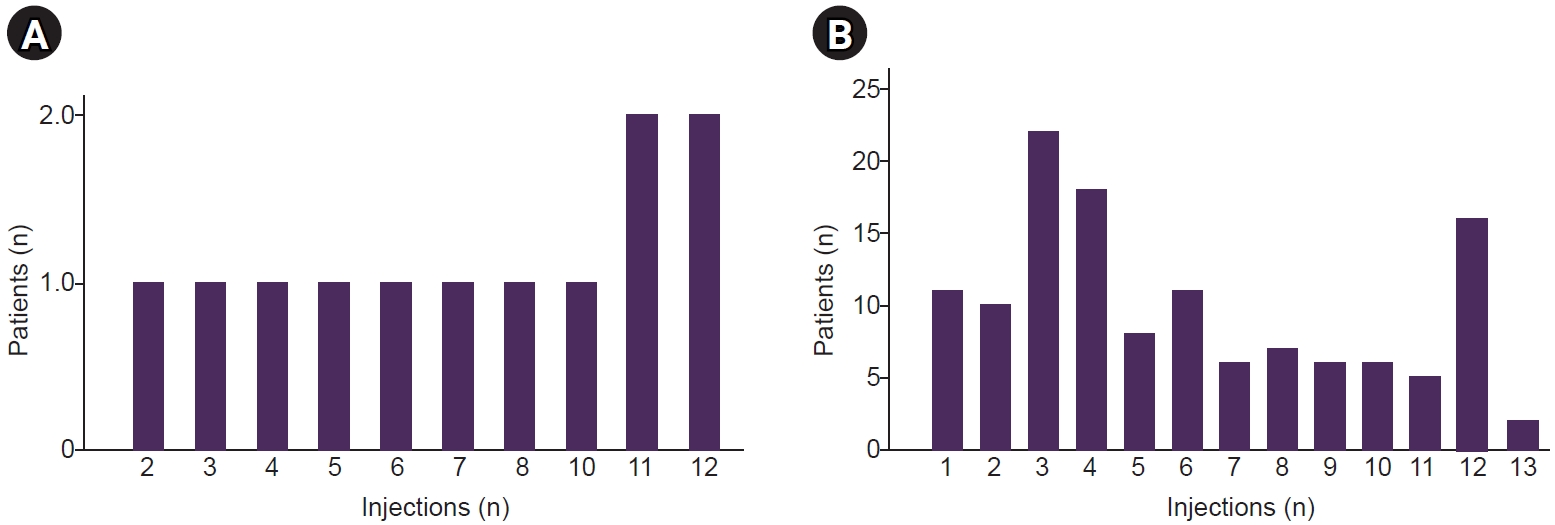
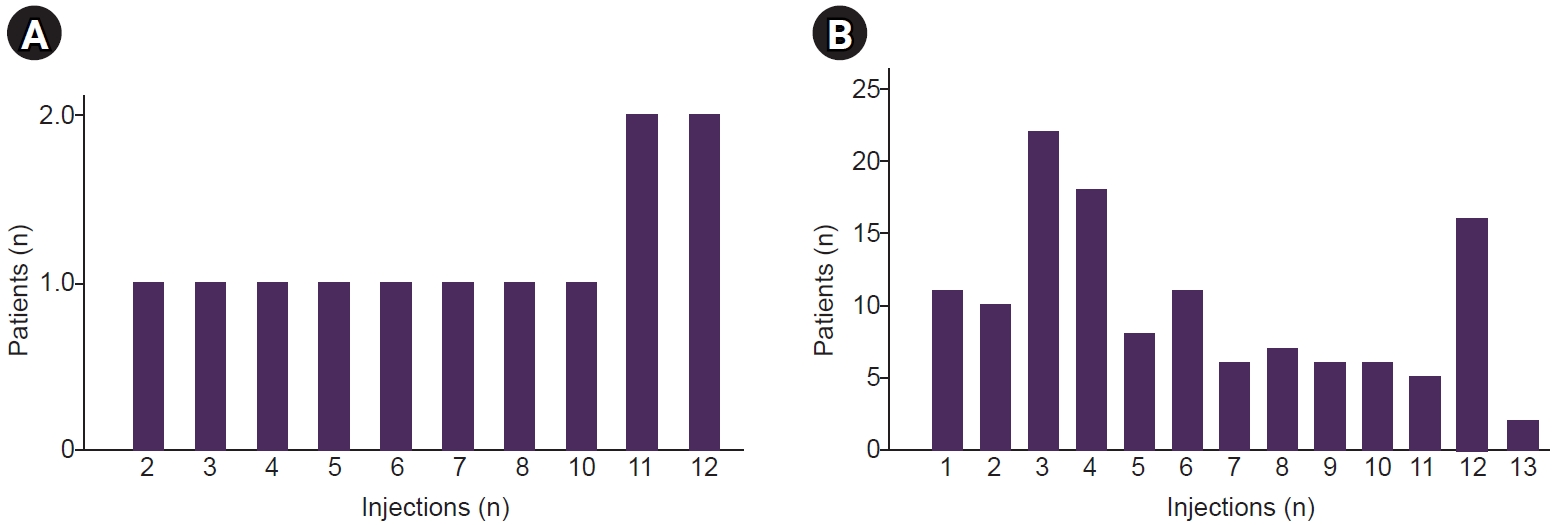
Figure 1.
| NHIS-covered (n=12) | Non-covered (n=128) | p-value | |
|---|---|---|---|
| Age (yr) | 43.6±15.7 | 44.7±11.8 | 0.902 |
| Sex, female | 10 (83.3) | 106 (82.8) | 0.662 |
| BMI (kg/m2) | 22.7±4.2 | 22.2±3.3 | 0.783 |
| Hypertension | 4 (33.3) | 13 (10.2) | 0.060 |
| DM | 0 | 3 (2.3) | 0.637 |
| Migraine subtype | |||
| Chronic migraine | 11 (91.7) | 80 (62.5) | 0.057 |
| Episodic migraine | 1 (8.3) | 48 (37.5) | |
| Without aura | 11 (91.7) | 120 (93.8) | 0.565 |
| With aura | 1 (8.3) | 8 (6.3) | |
| PMM | 0 | 7/123 (5.7) | 0.540 |
| MRM | 0 | 12/123 (9.8) |
|
| Baseline headache characteristics | |||
| Monthly headache days | 25.5 (14.0–28.0) | 15.0 (10.0–20.0) | 0.027 |
| Monthly medication days | 13.0 (3.0–25.0) | 10.0 (6.0–20.0) | 0.856 |
| Monthly headache days more than 26 | 6 (50.0) | 23 (18.0) | 0.018 |
| Age of onset (yr) | 20.9±10.3 | 27.1±12.7 | 0.152 |
| Disease duration before CGRP (yr) | 19.2±20.0 | 15.9±11.2 | 0.876 |
| Questionnaires | |||
| HIT-6 | 60.9±7.9 | 61.4±7.8 | 0.654 |
| GAD-7 | 5.5 (2.8‒9.8) | 5.0 (2.0‒8.8) | 0.436 |
| PHQ-9 | 8.5 (5.0‒13.3) | 7.0 (4.0‒9.0) | 0.150 |
| Anti-CGRP mAb type | |||
| Galcanezumab | 6 (50.0) | 53 (41.4) | 0.792 |
| Fremanezumab | 6 (50.0) | 75 (58.6) | |
| Prior anti-CGRP mAb treatment | 3 (25.0) | 23 (18.0) | 0.391 |
| NHIS-covered (n=12) | Non-covered (n=128) | p-value | |
|---|---|---|---|
| Total number of injections | 7.5 (4.3‒11.0) | 5.0 (3.0‒9.0) | 0.140 |
| Interval between injections (day) | 32.1 (30.7‒33.9) | 31.9 (30.0‒36.0) | 0.867 |
| Anti-CGRP mAb discontinuation | 6 (50.0) | 94 (73.4) | 0.101 |
| Reasons for discontinuation | |||
| Lack of effectiveness | 4/6 (66.7) | 17/94 (18.1) | |
| Headache improvement | 2/6 (33.3) | 30/94 (31.9) | |
| Loss of follow-up | - | 33/94 (35.1) | |
| Adverse events |
- | 7/94 (7.4) | |
| Financial reasons | - | 3/94 (3.2) | |
| Others | - | 4/94 (4.3) | |
| Overall adverse events | 2/12 (16.7) | 17/128 (13.3) | 0.667 |
| Adherence | 86.7 (57.5‒100) | 79.9 (43.3‒100) | 0.300 |
| Days covered | 225 (127.5‒330.0) | 150 (90.0‒270.0) | 0.140 |
| Adherent | 8 (66.7) | 64 (50.0) | 0.369 |
| Persistence | |||
| Duration of treatment (day) | 313.0 (120.3‒374.0) | 177.0 (91.3‒358.7) | 0.214 |
| At 6 months | |||
| Follow-up | 10 (83.8) | 100 (78.1) | >0.99 |
| Persistence rate | 8/10 (80.0) | 66/100 (66.0) | 0.493 |
| At 12 months | |||
| Follow-up | 9 (75.0) | 72 (56.2) | 0.240 |
| Persistence rate | 6/9 (66.7) | 34/72 (47.2) | 0.312 |
| Variable | MHD, mean±SD | ||||
|---|---|---|---|---|---|
| Baseline | After 1 month | After 3 months | After 6 months | After 12 months | |
| NHIS coverage | |||||
| Covered (n=12) | 21.7±8.0 | 16.4±10.6 | 15.3±10.4 | 14.6±10.6 | 10.9±10.4 |
| Non-covered (n=128) | 15.7±8.3 | 9.1±9.1 | 8.1±8.0 | 7.5±6.9 | 7.8±7.4 |
| p-value | 0.026 | 0.005 | 0.012 | 0.071 | 0.407 |
| Reduction in MHD from baseline | |||||
| Covered | 5.3±7.5 | 6.3±9.8 | 5.3±12.6 | 10.6±10.1 | |
| Non-covered | 6.0±7.5 | 6.8±7.8 | 7.6±7.3 | 7.7±9.0 | |
| p-value |
0.398 | 0.631 | 0.523 | 0.6 | |
| Treatment discontinuation | |||||
| Continued (n=40) | 15.6±6.8 | 8.2±7.7 | 8.9±7.9 | 8.4±6.9 | 6.7±5.3 |
| Discontinued (n=100) | 16.5±8.9 | 10.9±10.3 | 9.1±9.1 | 8.1±8.1 | 10.0±9.9 |
| p-value | 0.709 | 0.253 | 0.732 | 0.381 | 0.469 |
| Reduction in MHD from baseline | |||||
| Continued | 6.9±6.7 | 6.9±7.3 | 7.1±8.1 | 8.9±7.4 | |
| Discontinued | 5.4±8.3 | 6.3±8.5 | 7.6±7.9 | 7.0±10.8 | |
| p-value |
0.255 | 0.724 | 0.925 | 0.291 | |
Values are presented as mean±standard deviation, number (%), or median (interquartile range). anti-CGRP mAb, anti-calcitonin gene-related peptide monoclonal antibody; NHIS, National Health Insurance Service; BMI, body mass index; DM, diabetes mellitus; PMM, pure menstrual migraine; MRM, menstrual-related migraine; CGRP, calcitonin gene-related peptide; HIT-6, Headache Impact Test-6; GAD-7, Generalized Anxiety Disorder 7-Item Scale; PHQ-9, Patient Health Questionnaire-9. PMM and MRM analyses were performed in 123 patients in the non-covered group because data were unavailable for 5 patients.
Values are presented as median (interquartile range) or number (%). NHIS, National Health Insurance Service; Anti-CGRP mAb, anti-calcitonin gene-related peptide monoclonal antibody. Including allergic reactions (n=3), constipation (n=1), weight gain (n=1), vomiting (n=1), and abnormal uterine bleeding (n=1).
MHD, monthly headache days; SD, standard deviation. p-values represent between-group comparisons at each time point.
Table 1.
Table 2.
Table 3.
TOP

