Serum Triglyceride Levels in Pediatric Migraine and Tension-Type Headache: A Retrospective Study
Article information

Abstract
Purpose
Migraine and tension-type headache (TTH) are the most common primary headache disorders in children. However, potential metabolic differences between these conditions remain incompletely understood.
Methods
This retrospective study included pediatric patients diagnosed with migraine or TTH. Clinical characteristics and laboratory parameters were compared between the groups. Serum triglyceride (TG) levels were analyzed using multivariable linear regression adjusted for age and sex. Additional analyses included body mass index (BMI)-adjusted models and logarithmically transformed TG analyses.
Results
In total, 139 patients were included: 85 with migraine and 54 with TTH. Serum TG data were available for 101 patients. Mean TG levels were significantly higher in patients with TTH than in those with migraine (130.7±80.4 mg/dL vs. 92.1±42.4 mg/dL, p=0.006). This association remained significant after adjustment for age and sex (β=36.61 mg/dL, p=0.004), after logarithmic transformation (p=0.006), and in the BMI-adjusted subgroup analysis (β=42.84 mg/dL, p=0.040).
Conclusion
This exploratory retrospective study identified higher serum TG levels in pediatric patients with TTH than in those with migraine. Given the retrospective design and potential for residual confounding, these findings should be considered hypothesis-generating and require confirmation in prospective studies.
INTRODUCTION
Migraine and tension-type headache (TTH) are the most common primary headache disorders in children and adolescents.1,2 Diagnostic classification is based on the International Classification of Headache Disorders, 3rd edition (ICHD-3).1
Previous studies have suggested that metabolic factors, including obesity and lipid abnormalities, may be associated with primary headache disorders.3-5 Although several adult studies have investigated relationships between migraine and lipid profiles, pediatric data remain limited, and direct comparisons between headache subtypes are scarce.6
Serum triglyceride (TG) levels may reflect metabolic and lifestyle-related factors such as obesity, dietary patterns, physical inactivity, and stress-related metabolic changes.7-10 However, whether TG levels differ between pediatric migraine and TTH has not been well investigated.
The aim of this study was to compare clinical and laboratory characteristics between pediatric patients with migraine and TTH, with particular focus on serum TG levels.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board (IRB) of Wonju Severance Christian Hospital (IRB No. CR325073).
This retrospective study included pediatric patients aged 5–18 years diagnosed with migraine or TTH at a single tertiary medical center. Diagnoses were based on established clinical criteria according to ICHD-3. All diagnoses were made by a pediatric neurologist based on clinical evaluation according to ICHD-3 criteria. Both migraine with and without aura were included. Patients with chronic TTH were also eligible for inclusion. Patients with secondary headache or known metabolic disorders were excluded.
Laboratory evaluation was considered for pediatric patients presenting with primary headache. Serum lipid profiles were primarily obtained in the outpatient setting under recommended fasting conditions.11 Patients and guardians were instructed to visit after fasting, and when fasting status was not appropriate at the initial visit, laboratory testing including lipid profiles was deferred to another outpatient visit. Patients presenting through the emergency department generally did not undergo lipid profile testing because fasting conditions could not be ensured. However, because of the retrospective study design, strict adherence to fasting instructions could not be fully verified in all patients. All laboratory measurements were performed in the same institutional laboratory using standardized assays throughout the study period.
Lipid profile data were unavailable in some patients because of emergency department presentation, non-fasting status without subsequent testing, or patient/guardian refusal. Therefore, missing TG data were mainly related to visit setting, fasting feasibility, and consent for blood testing rather than selective testing based on headache severity.
Continuous variables are presented as mean±standard deviation, and categorical variables are presented as frequencies and percentages. Group comparisons were performed using Student’s t-test or chi-square test, as appropriate.
Serum TG levels were analyzed as the primary metabolic parameter of interest. Because TG values demonstrated right-skewed distribution, additional analyses using logarithmically transformed TG values were performed.
Multivariable linear regression analysis was conducted to evaluate the association between headache type and TG levels after adjustment for age and sex. Additional sensitivity analysis including body mass index (BMI) was performed in patients with available BMI data. TG-specific analyses were performed only in patients with available TG measurements (n=101).
RESULTS
A total of 139 patients were included in the study, including 85 patients with migraine and 54 patients with TTH. Serum TG levels were available in 101 patients, including 58 patients with migraine and 43 patients with TTH. Missing lipid profile data were primarily related to emergency department presentation without fasting conditions or absence of outpatient lipid testing. Patients without available TG measurements were older and more frequently female compared with those with available TG measurements; however, migraine/TTH distribution and BMI did not significantly differ between groups (Supplementary Table 1, available online).
Baseline clinical characteristics are summarized in Table 1. Patients with migraine were older than those with TTH, whereas sex distribution and BMI did not differ significantly between groups.
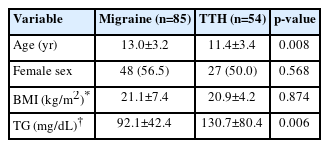
Baseline characteristics of pediatric patients with migraine and TTH
Mean serum TG levels were significantly higher in patients with TTH compared with migraine (130.7±80.4 mg/dL vs. 92.1±42.4 mg/dL, p=0.006) (Figure 1).
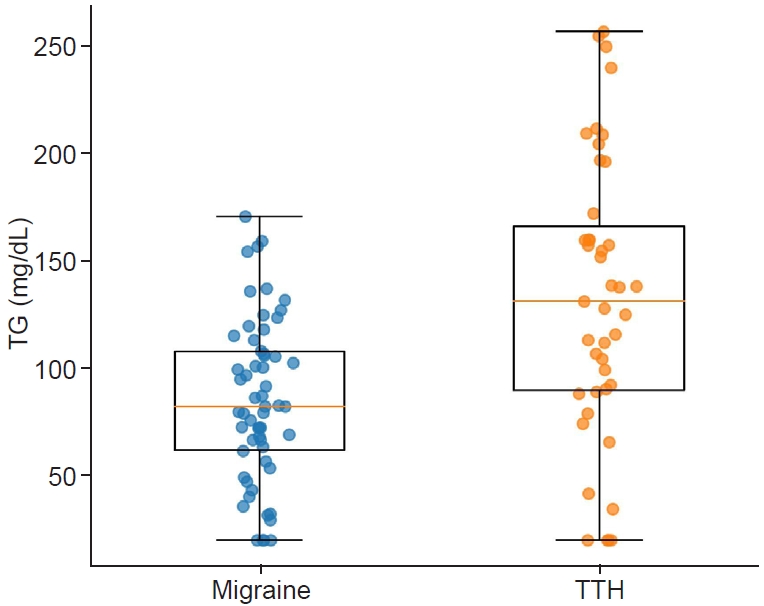
Distribution of serum triglyceride (TG) levels in pediatric patients with migraine and tension-type headache (TTH). TG levels were significantly higher in patients with TTH compared with migraine (p=0.006).
In multivariable linear regression analysis adjusted for age and sex, TTH remained significantly associated with higher TG levels (β=36.61 mg/dL, p=0.004) (Table 2).
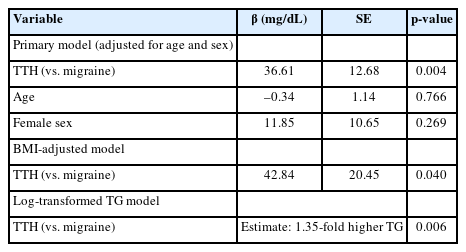
Multivariable analyses for serum TG levels
As the TG values showed a right-skewed distribution, an additional analysis was performed using the log-transformed TG values. The association between TTH and higher TG levels remained significant (Table 2).
In the subgroup with available BMI data, the association between TTH and higher TG levels also remained significant even after further adjustment for BMI (Table 2). In an exploratory analysis using age 12 years as a surrogate cutoff for pubertal status, the direction of the association between TTH and higher TG levels was generally consistent across age groups, although statistical significance was observed only in the younger subgroup and no significant interaction by age group was identified.
DISCUSSION
In this exploratory retrospective study, pediatric patients with TTH demonstrated significantly higher serum TG levels compared with patients with migraine. This association remained significant after adjustment for age, sex, and BMI, as well as after logarithmic transformation of TG values.
Several mechanisms may potentially explain this observation. Lifestyle-related factors such as dietary habits, physical inactivity, psychosocial stress, sleep disturbance, and obesity-related metabolic changes may contribute differently across headache subtypes.7-10 Irregular meal patterns, sedentary behavior, increased consumption of high-calorie foods, and obesity-related insulin resistance may also contribute to elevated TG levels in some pediatric patients with TTH. Previous studies have suggested associations between metabolic dysregulation and primary headache disorders, particularly migraine;3-5 however, direct comparisons between pediatric headache subtypes remain limited.6
The present findings should be interpreted cautiously. Although higher TG levels were observed in TTH, the clinical significance of this difference remains uncertain, and serum TG cannot currently be considered a diagnostic biomarker for differentiating headache subtypes.
Several limitations should be acknowledged. First, because of the retrospective single-center design, residual confounding and selection-related bias cannot be fully excluded. Although lipid profile testing was not selectively restricted to patients with more severe headache symptoms, TG data were unavailable in a subset of patients because of emergency department presentation, lack of fasting status, or refusal of blood sampling. Second, although outpatient lipid testing was generally performed after recommended fasting, actual adherence to fasting instructions could not be objectively confirmed. In addition, although age and sex differences were observed between patients with and without available TG measurements, multivariable analyses were adjusted for these variables. Third, additional metabolic confounders such as dietary patterns, physical activity, insulin resistance, and socioeconomic factors were not available for analysis. In addition, because pubertal status data were unavailable in this retrospective dataset, age-based subgroup analysis was used only as an exploratory surrogate and should be interpreted cautiously. Finally, the relatively small sample size limits definitive interpretation of subgroup analyses.
Recent domestic literature has also emphasized the growing clinical importance of pediatric headache disorders and the need for broader investigation of associated clinical factors.12
These findings may provide preliminary evidence supporting possible metabolic differences between pediatric headache subtypes and warrant further prospective studies with standardized metabolic assessment.
Notes
AVAILABILITY OF DATA AND MATERIAL
The data presented in this study are available upon reasonable request from the corresponding author.
AUTHOR CONTRIBUTIONS
Conceptualization: KTO; Data curation: KTO; Formal analysis: KTO; Investigation: KTO; Methodology: KTO; Project administration: KTO; Resources: KTO; Software: KTO; Supervision: KTO; Validation: KTO; Visualization: KTO; Writing–original draft: KTO; Writing–review & editing: KTO.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING STATEMENT
None.
ACKNOWLEDGMENTS
None.
SUPPLEMENTARY MATERIAL
Supplementary materials are available from https://doi.org/10.62087/hpr.2026.0016.
Comparison of baseline characteristics according to TG availability