
Articles
- Page Path
- HOME > Headache Pain Res > Volume 27(2); 2026 > Article
-
Original Article
Serum Triglyceride Levels in Pediatric Migraine and Tension-Type Headache: A Retrospective Study -
Ki Taek Oh

-
Headache and Pain Research 2026;27(2):154-157.
DOI: https://doi.org/10.62087/hpr.2026.0016
Published online: June 30, 2026
Department of Pediatrics, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Republic of Korea
- Correspondence: Ki Taek Oh, M.D. Department of Pediatrics, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, 20 Ilsan-ro, Wonju 26426, Republic of Korea Tel: +82-33-741-0114, E-mail: ohgt90@naver.com
© 2026 The Korean Headache Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 95 Views
- 2 Download
Abstract
-
Purpose
- Migraine and tension-type headache (TTH) are the most common primary headache disorders in children. However, potential metabolic differences between these conditions remain incompletely understood.
-
Methods
- This retrospective study included pediatric patients diagnosed with migraine or TTH. Clinical characteristics and laboratory parameters were compared between the groups. Serum triglyceride (TG) levels were analyzed using multivariable linear regression adjusted for age and sex. Additional analyses included body mass index (BMI)-adjusted models and logarithmically transformed TG analyses.
-
Results
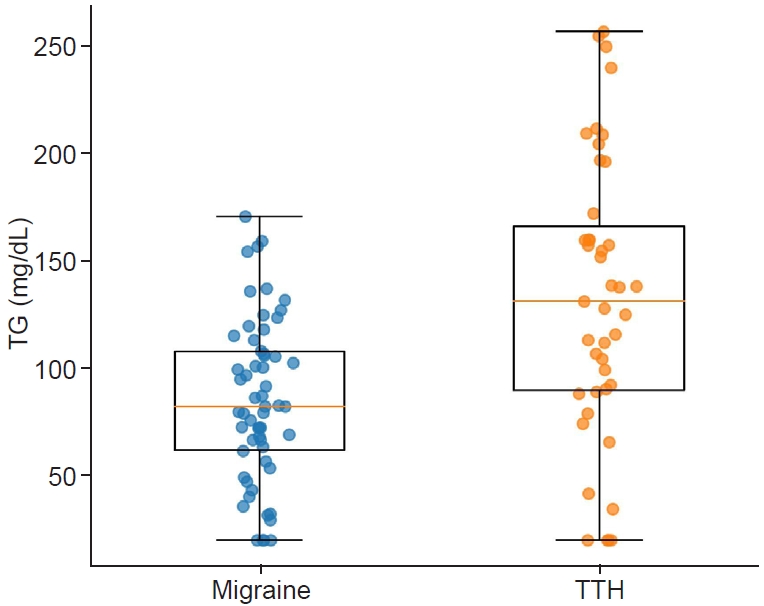
- In total, 139 patients were included: 85 with migraine and 54 with TTH. Serum TG data were available for 101 patients. Mean TG levels were significantly higher in patients with TTH than in those with migraine (130.7±80.4 mg/dL vs. 92.1±42.4 mg/dL, p=0.006). This association remained significant after adjustment for age and sex (β=36.61 mg/dL, p=0.004), after logarithmic transformation (p=0.006), and in the BMI-adjusted subgroup analysis (β=42.84 mg/dL, p=0.040).
-
Conclusion
- This exploratory retrospective study identified higher serum TG levels in pediatric patients with TTH than in those with migraine. Given the retrospective design and potential for residual confounding, these findings should be considered hypothesis-generating and require confirmation in prospective studies.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
AVAILABILITY OF DATA AND MATERIAL
The data presented in this study are available upon reasonable request from the corresponding author.
AUTHOR CONTRIBUTIONS
Conceptualization: KTO; Data curation: KTO; Formal analysis: KTO; Investigation: KTO; Methodology: KTO; Project administration: KTO; Resources: KTO; Software: KTO; Supervision: KTO; Validation: KTO; Visualization: KTO; Writing–original draft: KTO; Writing–review & editing: KTO.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING STATEMENT
None.
ACKNOWLEDGMENTS
None.
SUPPLEMENTARY MATERIAL
Supplementary Table 1.
| Variable | Migraine (n=85) | TTH (n=54) | p-value |
|---|---|---|---|
| Age (yr) | 13.0±3.2 | 11.4±3.4 | 0.008 |
| Female sex | 48 (56.5) | 27 (50.0) | 0.568 |
| BMI (kg/m2)* | 21.1±7.4 | 20.9±4.2 | 0.874 |
| TG (mg/dL)† | 92.1±42.4 | 130.7±80.4 | 0.006 |
- 1. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018;38:1-211.ArticlePubMedPMCPDF
- 2. Abu-Arafeh I, Razak S, Sivaraman B, Graham C. Prevalence of headache and migraine in children and adolescents: a systematic review of population-based studies. Dev Med Child Neurol 2010;52:1088-1097.ArticlePubMed
- 3. Goadsby PJ, Holland PR, Martins-Oliveira M, Hoffmann J, Schankin C, Akerman S. Pathophysiology of migraine: a disorder of sensory processing. Physiol Rev 2017;97:553-622.ArticlePubMedPMC
- 4. Ashina M. Migraine. N Engl J Med 2020;383:1866-1876.ArticlePubMed
- 5. Bigal ME, Rapoport AM. Obesity and chronic daily headache. Curr Pain Headache Rep 2012;16:101-109.ArticlePubMedPDF
- 6. Baglioni V, Orecchio S, Esposito D, Faedda N, Natalucci G, Guidetti V. Tension-type headache in children and adolescents. Life (Basel) 2023;13:825.Article
- 7. Hershey AD, Powers SW, Nelson TD, et al. Obesity in the pediatric headache population: a multicenter study. Headache 2009;49:170-177.ArticlePubMed
- 8. Pinhas-Hamiel O, Frumin K, Gabis L, et al. Headaches in overweight children and adolescents referred to a tertiary-care center in Israel. Obesity (Silver Spring) 2008;16:659-663.ArticlePubMedPDF
- 9. Robberstad L, Dyb G, Hagen K, Stovner LJ, Holmen TL, Zwart JA. An unfavorable lifestyle and recurrent headaches among adolescents: the HUNT study. Neurology 2010;75:712-717.ArticlePubMed
- 10. Oakley CB, Scher AI, Recober A, Peterlin BL. Headache and obesity in the pediatric population. Curr Pain Headache Rep 2014;18:416.ArticlePubMedPMCPDF
- 11. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents; National Heart, Lung, and Blood Institute. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report. Pediatrics 2011;128 Suppl 5:S213-S256.ArticlePubMedPMCPDF
- 12. Lee YJ. Pediatric headache in Korea: beyond a common complaint to a chronic neurological condition. Headache Pain Res 2026;27:4-6.ArticlePDF
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-

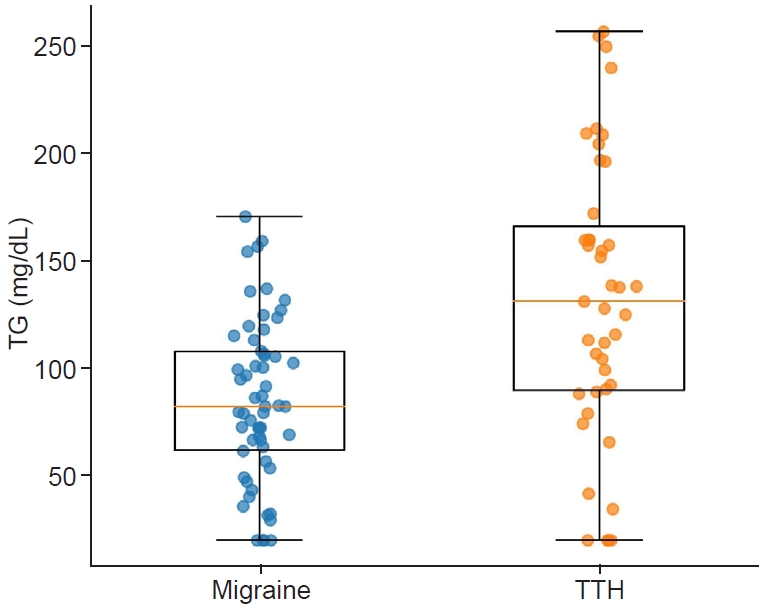
Figure 1.
| Variable | Migraine (n=85) | TTH (n=54) | p-value |
|---|---|---|---|
| Age (yr) | 13.0±3.2 | 11.4±3.4 | 0.008 |
| Female sex | 48 (56.5) | 27 (50.0) | 0.568 |
| BMI (kg/m2) |
21.1±7.4 | 20.9±4.2 | 0.874 |
| TG (mg/dL) |
92.1±42.4 | 130.7±80.4 | 0.006 |
| Variable | β (mg/dL) | SE | p-value |
|---|---|---|---|
| Primary model (adjusted for age and sex) | |||
| TTH (vs. migraine) | 36.61 | 12.68 | 0.004 |
| Age | –0.34 | 1.14 | 0.766 |
| Female sex | 11.85 | 10.65 | 0.269 |
| BMI-adjusted model | |||
| TTH (vs. migraine) | 42.84 | 20.45 | 0.040 |
| Log-transformed TG model | |||
| TTH (vs. migraine) | Estimate: 1.35-fold higher TG | 0.006 | |
Values are presented as mean±standard deviation or number (%). TTH, tension-type headache; BMI, body mass index; TG, triglyceride. BMI data were available in 27 patients with migraine and 29 patients with TTH. TG data were available in 58 patients with migraine and 43 patients with TTH.
TG, triglyceride; TTH, tension-type headache; BMI, body mass index; SE, standard error.
Table 1.
Table 2.
TOP

