
Articles
- Page Path
- HOME > Headache Pain Res > Volume 26(3); 2025 > Article
-
Original Article
Trigeminal Autonomic Cephalalgias Following Unilateral Dorsolateral Medullary Infarction: A Case Series and Literature Review -
Jae-Myung Kim
 , Hak-Loh Lee, You-Ri Kang, Joon-Tae Kim, Seung-Han Lee
, Hak-Loh Lee, You-Ri Kang, Joon-Tae Kim, Seung-Han Lee -
Headache and Pain Research 2025;26(3):218-225.
DOI: https://doi.org/10.62087/hpr.2025.0013
Published online: October 22, 2025
Department of Neurology, Chonnam National University Hospital, Chonnam National University Medical School, Gwangju, Republic of Korea
- Correspondence: Seung-Han Lee, M.D., Ph.D. Department of Neurology, Chonnam National University Hospital, 42 Jebong-ro, Dong-gu, Gwangju 61469, Republic of Korea Tel: +82-62-220-6274, Fax: +82-62-228-3461, E-mail: nrshlee@chonnam.ac.kr
© 2025 The Korean Headache Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,945 Views
- 28 Download
- 1 Crossref
Abstract
-
Purpose
- Secondary trigeminal autonomic cephalalgias (TACs) are typically associated with posterior fossa abnormalities, such as tumors and vascular malformations. However, TACs following brainstem infarctions are rarely reported. This study aimed to characterize the clinical and anatomical features of TACs after unilateral dorsolateral medullary infarction.
-
Methods
- We analyzed four patients with dorsolateral medullary infarction who developed secondary TACs, diagnosed using the International Classification of Headache Disorders, third edition criteria. All patients underwent detailed neurological examinations and neuroimaging, including diffusion-weighted magnetic resonance imaging and magnetic resonance angiography. Additionally, five published cases were identified through a literature review and analyzed in conjunction with our cohort.
-
Results
- All patients exhibited stabbing or electric shock-like pain in the ipsilateral periorbital, hemifacial, and temporal regions. Headaches developed weeks to months post-stroke with brief attacks (1–2 minutes) occurring 1–5 times daily. Lacrimation and conjunctival injection were common. Three patients were diagnosed with short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT), while a fourth had short-lasting unilateral neuralgiform with cranial autonomic symptoms (SUNA). Each patient, as well as four of the five from the literature, exhibited ipsilateral facial sensory loss, suggesting involvement of the trigeminal spinal tract and nucleus. Delayed headache onset was more frequent in persistent cases.
-
Conclusion
- Headache characteristics were more consistent with SUNCT/SUNA than with typical cluster headaches. Careful neurological examination is essential to detect focal signs and guide neuroimaging for identifying secondary causes. Clinicians should consider secondary TACs in patients with new-onset SUNCT/SUNA and focal brainstem signs.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
AVAILABILITY OF DATA AND MATERIAL
The data presented in this study are available upon reasonable request from the corresponding author.
AUTHOR CONTRIBUTIONS
Conceptualization: JMK, SHL; Data curation: JMK, HLL, YRK, JTK; Formal analysis: SHL; Investigation: JMK, HLL, YRK, JTK; Validation: SHL; Writing–original draft: JMK, SHL; Writing–review & editing: JMK, HLL, YRK, JTK, SHL.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING STATEMENT
Not applicable.
ACKNOWLEDGMENTS
Not applicable.
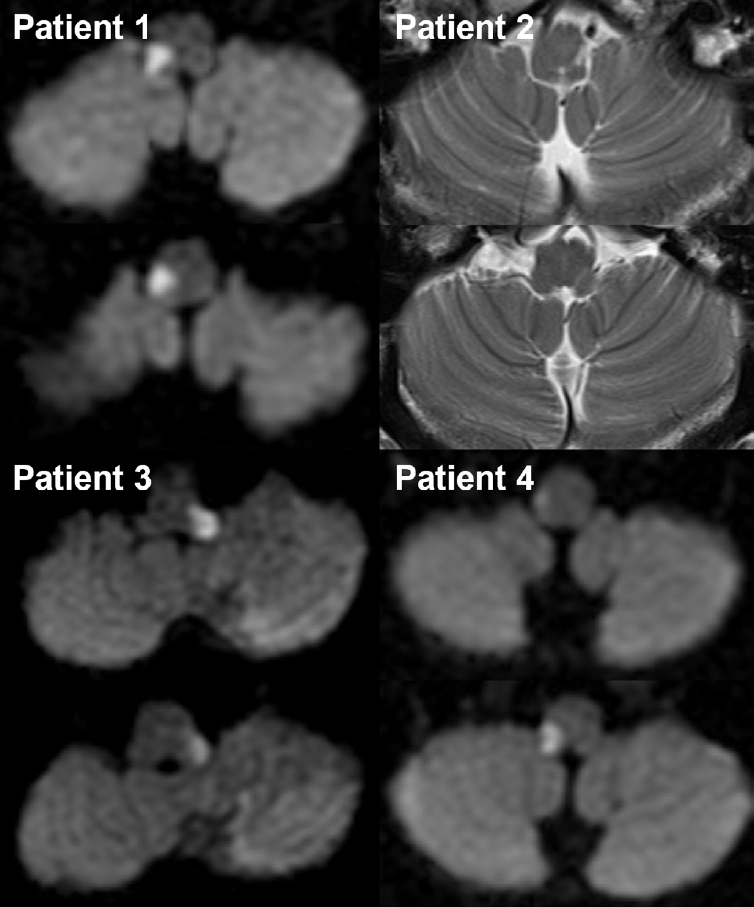
Neuroimaging of the four patients who presented with dorsolateral medullary infarction.
SUNCT, short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA, short-lasting unilateral neuralgiform with cranial autonomic symptoms; ICHD-3, International Classification of Headache Disorders, third edition; SNUHA, short-lasting unilateral neuralgiform headache attacks.
| Case | Age (yr) | Sex | Index stroke | Headache characteristics | Diagnosis of headache (ICHD-3) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Risk factor | TOAST | Angiography | MRI lesion | Associated neurological signs | Onset after stroke | Side | Location | Duration | Nature | Frequency (times) | Outcome | Autonomic symptoms | ||||
| Present cases | ||||||||||||||||
| Patient 1 | 70 | Male | HTN, DL | SVO | Normal | Rt. LMI | SL (i-F and c-B), AT (i-L and T), hoarseness | 3 mo | i | Periorbital, hemifacial, and temporal | 1–2 min | Stabbing | 3–4/day | Persistent | LC, CI, rhinorrhea | SUNCT |
| Patient 2 | 57 | Male | SVO | VA hypoplasia | Lt. LMI | SL (i-F and c-B), DysP, AT (i-L), vertigo, NY | 2.5 mo | i | Periorbital, hemifacial, and temporal | 1–2 min | Stabbing | 1–5/day | Resolved after several years | LC, CI | SUNCT | |
| Patient 3 | 56 | Male | Lipid | LAA | VA severe stenosis | Lt. LMI | SL (i-F and c-B), AT (T), HS, vertigo, NY | 4 mo | i | Periorbital, hemifacial, and temporal | <1 min | Electric shock-like | 1–5/day | Persistent | LC, CI, nasal congestion | SUNCT |
| Patient 4 | 50 | Female | HTN, HCC, RA | SOD | VA dissection | Rt. LMI | SL (i-F and c-B), AT (i-L and T), HS, vertigo, NY | 2.5 mo | i | Periorbital, hemifacial, and temporal | <1 min | Electric shock-like | 1–5/day | Persistent | LC | SUNA |
| Published cases | ||||||||||||||||
| Rodrigues et al. (2007)12 | 54 | Male | HTN | N/A | N/A | Rt. LMI | SL (i-F and c-B), AT (i-T), DysA | 6 mo | i | Orbital | 20 sec | N/A | >10/hr | Persistent | LC, CI | SUNCT |
| Jin et al. (2016)6 | 64 | Male | HTN, DM | LAA | VA occlusion | Lt. LMI | SL (i-F), HS, AT (i-T), vertigo | 13 day | i | Periorbital | 3–10 sec | Stabbing | 1–4/day | Resolved after 19 days | LC, CI, rhinorrhea | SUNCT |
| Lambru et al. (2017)7 | 58 | Male | HTN | SOD | VA dissection | Rt. LMI (hemorrhagic) | N/A | 21 day | i | Periorbital–temporal radiating to cheek/jaw | 5–20 sec | Stabbing, sharp | 12–15 (up to 50–60)/day | Persistent | LC, CI, ptosis, eyelid edema, rhinorrhea | SUNCT and TN |
| Lei et al. (2020)11 | 44 | Male | None | LAA | VA stenosis | Rt. LMI | SL (i-F and c-B), DysP, DysA, hiccup, hoarseness, HS, AT (i-L and T), hemiparesis (i), NY, vertigo, gag reflex ↓ | 0 day* | i | Hemifacial, temporal, occipital | 10–180 sec | Tearing | >10/day | Resolved after 1 month | LC, CI, nasal congestion | SUNCT |
| Gadah et al. (2025)10 | ~40 | Male | None | N/A | N/A | Rt. LMI | SL (i-F; V1 and V2), hand numbness (i) | 4 day | i | Hemifacial | 1 min | Burning | >4/day | Improved after 1 month, but persisted until 1 year | LC, CI, nasal discharge, facial grimacing with facial edema | SUNCT |
| Total (n=9) | Male (n=8) | SL (i-F)=8 of 9 | 0 day*–6 mo | i (100%) | Persistent=5, resolved=4 | SUNCT=8, SUNA=1 | ||||||||||
TAC, trigeminal autonomic cephalalgia; TOAST, Trial of Org 10172 in Acute Stroke Treatment; MRI, magnetic resonance imaging; ICHD-3, International Classification of Headache Disorders, third edition; HTN, hypertension; DL, dyslipidemia; SVO, small vessel occlusion; Rt., right; LMI, lateral medullary infarction; SL, sensory loss; i, ipsilateral; F, face; c, contralateral; B, body; AT, ataxia; L, limb; T, trunk; LC, lacrimation; CI, conjunctival injection; SUNCT, short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; VA, vertebral artery; Lt., left; DysP, dysphagia; NY, nystagmus; LAA, large artery atherosclerosis; HS, Horner’s syndrome; HCC, hepatocellular carcinoma; RA, rheumatoid arthritis; SOD, stroke of other determined etiology; SUNA, short-lasting unilateral neuralgiform with cranial autonomic symptoms; N/A, not available; DysA, dysarthria; DM, diabetes mellitus; TN, trigeminal neuralgia.
*Same day as stroke onset.
| Group | Case (Ref.) | Headache onset after stroke | Headache duration | Diagnosis | Tx. regimen (max. daily dose) | Duration (mo) | Associated neurological signs |
|---|---|---|---|---|---|---|---|
| Persistent (n=5) | Patient 1 (this study) | 3 mo | Persistent | SUNCT | VER 80 mg/GBP 800 mg/LIT 600 mg/VPA 250 mg | 42/96/66/72 | SL (i-F and c-B), AT (i-L and T), hoarseness |
| Patient 3 (this study) | 4 mo | Persistent | SUNCT | VER 180 mg/AMI 5 mg/GBP 300 mg | 87/90/75 | SL (i-F and c-B), AT (T), HS, vertigo, NY | |
| Patient 4 (this study) | 2.5 mo | Persistent | SUNA | PGB 150 mg/GBP 800 mg | 74/118 | SL (i-F and c-B), AT (i-L and T), HS, vertigo, NY | |
| Rodrigues et al. (2007)12 | 6 mo | Persistent | SUNCT | VER*/CBZ*/LTG* | N/A | SL (i-F and c-B), AT (i-T), DysA | |
| Lambru et al. (2017)7 | 21 day | Persistent | SUNCT/TN | CBZ 800 mg/OXC 1,350 mg/GBP 900 mg/AMI 40 mg/LTG 50 mg/DLX 30 mg | N/A | N/A | |
| Mean | - | 3.24 mo | - | - | - | ||
| Resolved (n=4) | Patient 2 (this study) | 2.5 mo | Resolved | SUNCT | GBP 400 mg | 60 | SL (i-F and c-B), DysP, AT (i-L), vertigo, NY |
| Jin et al. (2016)6 | 13 day | Resolved | SUNCT | No Tx. | N/A | SL (i-F), HS, AT (i-T), vertigo | |
| Lei et al. (2020)11 | 0 day | Resolved | SUNCT | N/A | N/A | SL (i-F and c-B), DysP, DysA, hiccup, hoarseness, HS, AT (i-L and T), hemiparesis (i), NY, vertigo, gag reflex ↓ | |
| Gadah et al. (2025)10 | 4 day | Resolved | SUNCT | LTG* | 12 | SL (i-F; V1 and V2), hand numbness (i) | |
| Mean | - | 0.76 mo | - | - | - |
TAC, trigeminal autonomic cephalalgia; Ref., reference; Tx., treatment; max., maximum; SUNCT, short-lasting unilateral neuralgiform headache with conjunctival injection and tearing; VER, verapamil; GBP, gabapentin; LIT, lithium; VPA, valproic acid; SL, sensory loss; i, ipsilateral; F, face; c, contralateral; B, body; AT, ataxia; L, limb; T, trunk; AMI, amitriptyline; HS, Horner’s syndrome; NY, nystagmus; SUNA, short-lasting unilateral neuralgiform with cranial autonomic symptoms; PGB, pregabalin; CBZ, carbamazepine; LTG, lamotrigine; N/A, not available; DysA, dysarthria; OXC, oxcarbazepine; DLX, duloxetine; TN, trigeminal neuralgia; DysP, dysphagia.
*Exact medication doses were not reported in the original case reports.
- 1. Goadsby PJ, Lipton RB. A review of paroxysmal hemicranias, SUNCT syndrome and other short-lasting headaches with autonomic feature, including new cases. Brain 1997;120:193-209.ArticlePubMed
- 2. Cittadini E, Matharu MS. Symptomatic trigeminal autonomic cephalalgias. Neurologist 2009;15:305-312.ArticlePubMed
- 3. Liu J, Xiao S, Yang F, et al. Symptomatic trigeminal autonomic cephalalgias in neuromyelitis optica spectrum disorders. Mult Scler Relat Disord 2023;74:104722.ArticlePubMed
- 4. Kang MK, Cho SJ. SUNCT, SUNA and short-lasting unilateral neuralgiform headache attacks: debates and an update. Cephalalgia 2024;44:3331024241232256.ArticlePubMedPDF
- 5. Cao Y, Yang F, Dong Z, Huang X, Cao B, Yu S. Secondary short-lasting unilateral neuralgiform headache with conjunctival injection and tearing: a new case and a literature review. J Clin Neurol 2018;14:433-443.ArticlePDF
- 6. Jin D, Lian YJ, Zhang HF. Secondary SUNCT syndrome caused by dorsolateral medullary infarction. J Headache Pain 2016;17:12.ArticlePubMedPMCPDF
- 7. Lambru G, Trimboli M, Tan SV, Al-Kaisy A. Medullary infarction causing coexistent SUNCT and trigeminal neuralgia. Cephalalgia 2017;37:486-490.ArticlePubMedPDF
- 8. Ordás CM, Cuadrado ML, Simal P, et al. Wallenberg’s syndrome and symptomatic trigeminal neuralgia. J Headache Pain 2011;12:377-380.ArticlePubMedPMCPDF
- 9. Penart A, Firth M, Bowen JR. Short-lasting unilateral neuralgiform headache with conjunctival injection and tearing (SUNCT) following presumed dorsolateral brainstem infarction. Cephalalgia 2001;21:236-239.ArticlePubMedPDF
- 10. Gadah AA, AbaAlkhail AB, Khatri IA. Onset of secondary SUNCT syndrome with concomitant occipital neuralgia after dorsal medullary infarction. BMJ Case Rep 2025;18:e264684.ArticlePubMed
- 11. Lei Q, Lv J, Kang B, et al. Comorbid SUNCT syndrome and Opalski Syndrome caused by dorsolateral medullary infarction. Front Neurol 2020;11:52.ArticlePubMedPMC
- 12. Rodrigues GG, Bordini CA, Dach F, Eckeli A, Speciali JG. SUNCT syndrome: report of a possible symptomatic case. Arq Neuropsiquiatr 2007;65:852-854.ArticlePubMed
- 13. Galende AV, Camacho A, Gomez-Escalonilla C, et al. Lateral medullary infarction secondary to vertebral artery dissection presenting as a trigeminal autonomic cephalalgia. Headache 2004;44:70-74.ArticlePubMed
- 14. Kim JT, Lee SH, Choi SM, et al. Spontaneous vertebral artery dissection mimicking cluster headache. Cephalalgia 2008;28:671-673.ArticlePubMedPDF
- 15. Lambru G, Rantell K, Levy A, Matharu MS. A prospective comparative study and analysis of predictors of SUNA and SUNCT. Neurology 2019;93:e1127-e1137.ArticlePubMed
- 16. Lambru G, Zakrzewska J, Matharu M. Trigeminal neuralgia: a practical guide. Pract Neurol 2021;21:392-402.ArticlePubMedPMC
- 17. Liampas A, Velidakis N, Georgiou T, et al. Prevalence and management challenges in central post-stroke neuropathic pain: a systematic review and meta-analysis. Adv Ther 2020;37:3278-3291.ArticlePubMedPMCPDF
- 18. Altavilla R, Landi D, Altamura C, et al. Dorsolateral medullary ischemic infarction causing autonomic dysfunction and headache: a case report. J Headache Pain 2012;13:327-330.ArticlePubMedPMCPDF
- 19. Sessle BJ; International Association for the Study of Pain. Orofacial pain: recent advances in assessment, management, and understanding of mechanisms. IASP Press; 2014.
- 20. Kim M, Yu JK, Kim YH. Update on cluster headaches: from genetic to novel therapeutic approaches. Headache Pain Res 2024;25:42-53.ArticlePDF
- 21. May A, Bahra A, Büchel C, Frackowiak RS, Goadsby PJ. Hypothalamic activation in cluster headache attacks. Lancet 1998;352:275-278.ArticlePubMed
- 22. Pringsheim T. Cluster headache: evidence for a disorder of circadian rhythm and hypothalamic function. Can J Neurol Sci 2002;29:33-40.ArticlePubMed
- 23. May A, Schwedt TJ, Magis D, Pozo-Rosich P, Evers S, Wang SJ. Cluster headache. Nat Rev Dis Primers 2018;4:18006.ArticlePubMedPDF
- 24. Kim JS. Pure lateral medullary infarction: clinical-radiological correlation of 130 acute, consecutive patients. Brain 2003;126:1864-1872.ArticlePubMed
- 25. Chowdhury D. Secondary (symptomatic) trigeminal autonomic cephalalgia. Ann Indian Acad Neurol 2018;21:S57-S69.ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Primary or Secondary Headache Disorders in Moyamoya Disease and Cerebral Infarction: Clinical Challenges and the Potential Role of Non-Vasoconstrictive Migraine Therapies
Soo-Jin Cho
Headache and Pain Research.2026; 27(1): 1. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-

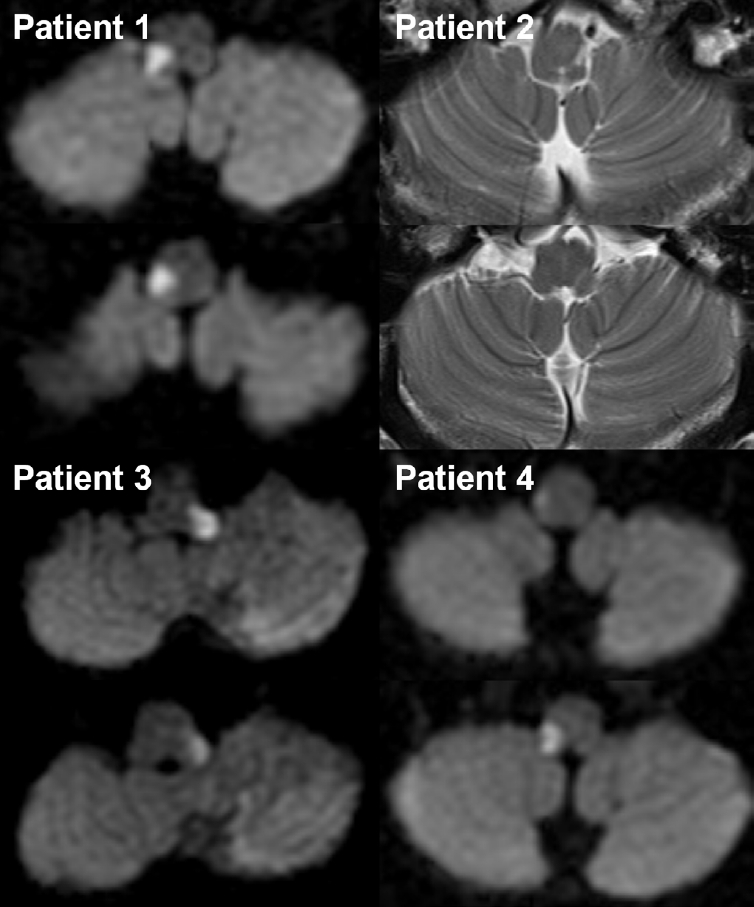
Figure 1.
| SNUHA |
| A. At least 20 attacks fulfilling criteria B–D |
| B. Moderate or severe unilateral head pain, with orbital, supraorbital, temporal, and/or other trigeminal distribution, lasting 1–600 seconds and occurring as single stabs, series of stabs, or in a saw-tooth pattern |
| C. At least one of the following five cranial autonomic symptoms or signs, ipsilateral to the pain: |
| 1. conjunctival injection and/or lacrimation |
| 2. nasal congestion and/or rhinorrhoea |
| 3. eyelid oedema |
| 4. forehead and facial sweating |
| 5. forehead and facial flushing |
| 6. sensation of fullness in the ear |
| 7. miosis and/or ptosis |
| D. Occurring with a frequency of at least once daily |
| E. Not better accounted for by another ICHD-3 diagnosis. |
| SUNCT |
| A. Attacks fulfilling criteria for SNUHA, and criterion B below |
| B. Both of the following are ipsilateral to the pain: |
| 1. conjunctival injection |
| 2. lacrimation (tearing) |
| SUNA |
| A. Attacks fulfilling criteria for SNUHA, and criterion B below |
| B. Only one or neither of conjunctival injection or lacrimation (tearing). |
| Case | Age (yr) | Sex | Index stroke | Headache characteristics | Diagnosis of headache (ICHD-3) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Risk factor | TOAST | Angiography | MRI lesion | Associated neurological signs | Onset after stroke | Side | Location | Duration | Nature | Frequency (times) | Outcome | Autonomic symptoms | ||||
| Present cases | ||||||||||||||||
| Patient 1 | 70 | Male | HTN, DL | SVO | Normal | Rt. LMI | SL (i-F and c-B), AT (i-L and T), hoarseness | 3 mo | i | Periorbital, hemifacial, and temporal | 1–2 min | Stabbing | 3–4/day | Persistent | LC, CI, rhinorrhea | SUNCT |
| Patient 2 | 57 | Male | SVO | VA hypoplasia | Lt. LMI | SL (i-F and c-B), DysP, AT (i-L), vertigo, NY | 2.5 mo | i | Periorbital, hemifacial, and temporal | 1–2 min | Stabbing | 1–5/day | Resolved after several years | LC, CI | SUNCT | |
| Patient 3 | 56 | Male | Lipid | LAA | VA severe stenosis | Lt. LMI | SL (i-F and c-B), AT (T), HS, vertigo, NY | 4 mo | i | Periorbital, hemifacial, and temporal | <1 min | Electric shock-like | 1–5/day | Persistent | LC, CI, nasal congestion | SUNCT |
| Patient 4 | 50 | Female | HTN, HCC, RA | SOD | VA dissection | Rt. LMI | SL (i-F and c-B), AT (i-L and T), HS, vertigo, NY | 2.5 mo | i | Periorbital, hemifacial, and temporal | <1 min | Electric shock-like | 1–5/day | Persistent | LC | SUNA |
| Published cases | ||||||||||||||||
| Rodrigues et al. (2007)12 | 54 | Male | HTN | N/A | N/A | Rt. LMI | SL (i-F and c-B), AT (i-T), DysA | 6 mo | i | Orbital | 20 sec | N/A | >10/hr | Persistent | LC, CI | SUNCT |
| Jin et al. (2016)6 | 64 | Male | HTN, DM | LAA | VA occlusion | Lt. LMI | SL (i-F), HS, AT (i-T), vertigo | 13 day | i | Periorbital | 3–10 sec | Stabbing | 1–4/day | Resolved after 19 days | LC, CI, rhinorrhea | SUNCT |
| Lambru et al. (2017)7 | 58 | Male | HTN | SOD | VA dissection | Rt. LMI (hemorrhagic) | N/A | 21 day | i | Periorbital–temporal radiating to cheek/jaw | 5–20 sec | Stabbing, sharp | 12–15 (up to 50–60)/day | Persistent | LC, CI, ptosis, eyelid edema, rhinorrhea | SUNCT and TN |
| Lei et al. (2020)11 | 44 | Male | None | LAA | VA stenosis | Rt. LMI | SL (i-F and c-B), DysP, DysA, hiccup, hoarseness, HS, AT (i-L and T), hemiparesis (i), NY, vertigo, gag reflex ↓ | 0 day |
i | Hemifacial, temporal, occipital | 10–180 sec | Tearing | >10/day | Resolved after 1 month | LC, CI, nasal congestion | SUNCT |
| Gadah et al. (2025)10 | ~40 | Male | None | N/A | N/A | Rt. LMI | SL (i-F; V1 and V2), hand numbness (i) | 4 day | i | Hemifacial | 1 min | Burning | >4/day | Improved after 1 month, but persisted until 1 year | LC, CI, nasal discharge, facial grimacing with facial edema | SUNCT |
| Total (n=9) | Male (n=8) | SL (i-F)=8 of 9 | 0 day |
i (100%) | Persistent=5, resolved=4 | SUNCT=8, SUNA=1 | ||||||||||
| Group | Case (Ref.) | Headache onset after stroke | Headache duration | Diagnosis | Tx. regimen (max. daily dose) | Duration (mo) | Associated neurological signs |
|---|---|---|---|---|---|---|---|
| Persistent (n=5) | Patient 1 (this study) | 3 mo | Persistent | SUNCT | VER 80 mg/GBP 800 mg/LIT 600 mg/VPA 250 mg | 42/96/66/72 | SL (i-F and c-B), AT (i-L and T), hoarseness |
| Patient 3 (this study) | 4 mo | Persistent | SUNCT | VER 180 mg/AMI 5 mg/GBP 300 mg | 87/90/75 | SL (i-F and c-B), AT (T), HS, vertigo, NY | |
| Patient 4 (this study) | 2.5 mo | Persistent | SUNA | PGB 150 mg/GBP 800 mg | 74/118 | SL (i-F and c-B), AT (i-L and T), HS, vertigo, NY | |
| Rodrigues et al. (2007)12 | 6 mo | Persistent | SUNCT | VER |
N/A | SL (i-F and c-B), AT (i-T), DysA | |
| Lambru et al. (2017)7 | 21 day | Persistent | SUNCT/TN | CBZ 800 mg/OXC 1,350 mg/GBP 900 mg/AMI 40 mg/LTG 50 mg/DLX 30 mg | N/A | N/A | |
| Mean | - | 3.24 mo | - | - | - | ||
| Resolved (n=4) | Patient 2 (this study) | 2.5 mo | Resolved | SUNCT | GBP 400 mg | 60 | SL (i-F and c-B), DysP, AT (i-L), vertigo, NY |
| Jin et al. (2016)6 | 13 day | Resolved | SUNCT | No Tx. | N/A | SL (i-F), HS, AT (i-T), vertigo | |
| Lei et al. (2020)11 | 0 day | Resolved | SUNCT | N/A | N/A | SL (i-F and c-B), DysP, DysA, hiccup, hoarseness, HS, AT (i-L and T), hemiparesis (i), NY, vertigo, gag reflex ↓ | |
| Gadah et al. (2025)10 | 4 day | Resolved | SUNCT | LTG |
12 | SL (i-F; V1 and V2), hand numbness (i) | |
| Mean | - | 0.76 mo | - | - | - |
SUNCT, short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA, short-lasting unilateral neuralgiform with cranial autonomic symptoms; ICHD-3, International Classification of Headache Disorders, third edition; SNUHA, short-lasting unilateral neuralgiform headache attacks.
TAC, trigeminal autonomic cephalalgia; TOAST, Trial of Org 10172 in Acute Stroke Treatment; MRI, magnetic resonance imaging; ICHD-3, International Classification of Headache Disorders, third edition; HTN, hypertension; DL, dyslipidemia; SVO, small vessel occlusion; Rt., right; LMI, lateral medullary infarction; SL, sensory loss; i, ipsilateral; F, face; c, contralateral; B, body; AT, ataxia; L, limb; T, trunk; LC, lacrimation; CI, conjunctival injection; SUNCT, short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; VA, vertebral artery; Lt., left; DysP, dysphagia; NY, nystagmus; LAA, large artery atherosclerosis; HS, Horner’s syndrome; HCC, hepatocellular carcinoma; RA, rheumatoid arthritis; SOD, stroke of other determined etiology; SUNA, short-lasting unilateral neuralgiform with cranial autonomic symptoms; N/A, not available; DysA, dysarthria; DM, diabetes mellitus; TN, trigeminal neuralgia. Same day as stroke onset.
TAC, trigeminal autonomic cephalalgia; Ref., reference; Tx., treatment; max., maximum; SUNCT, short-lasting unilateral neuralgiform headache with conjunctival injection and tearing; VER, verapamil; GBP, gabapentin; LIT, lithium; VPA, valproic acid; SL, sensory loss; i, ipsilateral; F, face; c, contralateral; B, body; AT, ataxia; L, limb; T, trunk; AMI, amitriptyline; HS, Horner’s syndrome; NY, nystagmus; SUNA, short-lasting unilateral neuralgiform with cranial autonomic symptoms; PGB, pregabalin; CBZ, carbamazepine; LTG, lamotrigine; N/A, not available; DysA, dysarthria; OXC, oxcarbazepine; DLX, duloxetine; TN, trigeminal neuralgia; DysP, dysphagia. Exact medication doses were not reported in the original case reports.
Table 1.
Table 2.
Table 3.
TOP

