Guideline for the Treatment of Cluster Headache: A Clinical Practice Guideline from the Korean Headache Society
Article information
 , Pil-Wook Chung,2, Hong-Kyun Park3, Mi Ji Lee4, Jae Myun Chung5, Kyung Min Kim6, Jiyoung Kim7, Heui-Soo Moon2, Dae-Woong Bae8, Jong-Hee Sohn9, Tae-Jin Song10, Wonwoo Lee11, Soohyun Cho12, Myoung-Jin Cha13, Yun-Ju Choi14, Miyoung Choi15, The Clinical Practice Guideline Committee of the Korean Headache Society
, Pil-Wook Chung,2, Hong-Kyun Park3, Mi Ji Lee4, Jae Myun Chung5, Kyung Min Kim6, Jiyoung Kim7, Heui-Soo Moon2, Dae-Woong Bae8, Jong-Hee Sohn9, Tae-Jin Song10, Wonwoo Lee11, Soohyun Cho12, Myoung-Jin Cha13, Yun-Ju Choi14, Miyoung Choi15, The Clinical Practice Guideline Committee of the Korean Headache SocietyAbstract
Purpose
This clinical practice guideline (CPG) was developed by the Korean Headache Society (KHS) to provide evidence-based recommendations for the acute and preventive treatment of cluster headache (CH).
Methods
The CPG Committee of the KHS identified key clinical questions regarding the acute and preventive treatment of CH through a systematic literature review. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology was used to assess the quality of evidence and determine the strength of the evidence-based recommendations.
Results
For acute treatment, subcutaneous sumatriptan, intranasal zolmitriptan, intranasal sumatriptan, oral zolmitriptan, and oxygen are strongly recommended based on moderate-quality evidence. For preventive treatment, suboccipital steroid injection, oral corticosteroids, and galcanezumab (specifically for episodic CH) are strongly recommended based on moderate-quality evidence. Despite the low quality of evidence, verapamil is also strongly recommended, whereas lithium is recommended with a weaker strength of recommendation. Other oral triptans, NSAIDs, ergot derivatives, subcutaneous octreotide, intranasal lidocaine, and non-invasive vagus nerve stimulation (nVNS; specifically for episodic CH) are recommended for acute treatment based on expert consensus. For preventive treatment, topiramate, valproic acid, melatonin, and nVNS (as adjunctive therapy specifically for chronic CH) are recommended, whereas sphenopalatine ganglion stimulation, occipital nerve stimulation, and deep brain stimulation are recommended for patients with refractory chronic CH based on expert consensus.
Conclusion
This CPG provides evidence-based recommendations for the treatment of CH. In addition, the authors recommend the use of expert consensus-based treatments to bridge the gap between the available evidence and real-world clinical practice.
INTRODUCTION
Cluster headache (CH) is a rare primary headache disorder, alongside migraine and tension-type headache, with an estimated prevalence of approximately 0.1%.1,2 Due to its low prevalence, patients with CH present less frequently to headache clinics and emergency departments compared to those with more common primary headache disorders such as migraine. Nevertheless, CH is widely recognized as one of the most severe pain conditions experienced by humans. Historically, CH has been referred to as the “suicide headache,” and a recent cohort study has reported an increased risk of suicidal ideation among affected patients.3
Despite the significant pain and disability associated with CH, advances in its treatment have been relatively limited. Similar to migraine management, the treatment of CH is generally divided into acute therapy, which aims to relieve the pain of CH attacks, and preventive therapy, which aims to reduce attack frequency and improve the response to acute treatments. In current clinical practice, both acute and preventive management of CH primarily relies on various oral medications traditionally used for migraine or other neurological disorders. Meanwhile, the development of anti–calcitonin gene-related peptide monoclonal antibodies (CGRP mAbs) and the successful clinical trial of preventive treatment for patients with episodic CH marked a major turning point in managing this disorder.4 In 2019, the U.S. Food and Drug Administration (FDA) approved galcanezumab as a preventive treatment for episodic CH. Compared to conventional oral preventive medications, anti-CGRP mAbs are expected to offer superior efficacy, fewer adverse effects, and better patient adherence, thereby significantly improving the management of CH.
Despite gradual advances in the diagnosis and treatment of CH, many patients continue to face significant challenges due to inadequate diagnosis and treatment. Therefore, the primary objective of developing this clinical practice guideline (CPG) is to provide practical guidance to support treatment decisions in clinical settings for managing CH, ultimately helping to reduce the disease burden among patients with CH.
MATERIALS AND METHODS
1. Design, participants, and users
The CPG Committee of the Korean Headache Society (KHS) developed the evidence-based recommendations on the treatment of CH using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology through a de novo approach.5 In cases where there was insufficient evidence or where a treatment was not readily applicable in the Korean healthcare setting, the decision on whether to recommend it was made through expert consensus. Therefore, this CPG was formulated into two parts. The first part of this CPG outlines evidence-based recommendations, while the second part provides statements based on expert consensus.
The CPG Committee consists of the Implementation Committee, the Development Committee, and the Oversight Committee. Within the Development Working Group (DWG), the Implementation Committee comprised five neurologists with expertise in CH, while the Development Committee included 10 neurologists and one guideline methodologist (M.C., National Evidence-based Healthcare Collaborating Agency). All CPG committee members had disclosed any conflict of interest that may potentially affect their participation and work. The DWG members have regularly communicated via e-mail and online meetings during the CPG development period.
The intended users for this CPG include primary care physicians, headache physicians, nurses, pharmacists, healthcare administrators, CH patients, and the general public.
This CPG will be reviewed and updated as necessary, with revisions planned at approximately 3-year intervals by the Implementation Committee of the KHS.
2. Formulation of key questions
In identifying the key questions (KQs), the DWG members took into account the fact that CH is rare and that a literature review revealed limited evidence from clinical trials regarding their treatment. The KQs for this CPG were formulated according to the Patient, Intervention, Comparison, and Outcome (PICO) framework.6 The Development Committee initially drafted the KQs and related search terms, which were then compiled by the Implementation Committee for review and selection. Following this, the Oversight Committee reviewed and approved them, leading to their final selection.
The selection of treatments relevant to the KQs raised by the Implementation Committee was determined by a vote of the committee members. Ultimately, two acute treatments (oxygen and triptans) and five preventive treatments (suboccipital steroid injection, oral steroids, verapamil, lithium, and anti-CGRP mAbs) were included in the KQs. However, given that the number of clinical trials on CH remains insufficient at this time and that the disease imposes a significant burden on patients due to severe pain and unmet medical needs, it was determined necessary to include not only evidence-based treatments addressing the KQs but also medications empirically effective in clinical practice and treatments unavailable in Korea. Accordingly, it was decided to include treatments not covered by the KQs as “expert consensus” in this CPG. The selection and exclusion of treatments to be included in the expert consensus section were determined through meetings and voting by the Implementation Committee.
3. Search and selection of literature
The literature search was conducted independently of the CPG committee using four databases: PubMed (MEDLINE), Embase, the Cochrane Library, and KoreaMed (last updated in September 2022). The search terms included “cluster headache”, specific treatment, as well as their combinations (e.g., “cluster headache” OR “sumatriptan”). The search for all KQs did not exclude any records based on year, language, or publication status; after the search was completed, the identified evidence was aggregated, and duplicates were excluded based on title, author name, publication year, and journal name. For all identified literatures, two Implementation Committee members were assigned to each KQ to ensure that duplicates were excluded; studies were selected following a content review, and the selection process was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. The search strategy is provided in Supplementary Table 1 (available online).
4. Analysis of evidence and recommendations
Risk of bias was assessed using the ROB2 (Cochrane’s Risk of Bias) assessment tool for randomized clinical trials.7 Regarding each KQ, the retrieved literatures were evaluated to determine the quality of evidence (QOE). We used the GRADE profiler (https://gradepro.org/) to generate “summary of findings” tables informing certainty assessment and treatment outcome with the QOE. The QOE was rated as follows: high, very confident in the estimated effect’s closeness to reality; moderate reasonably confident in the estimate, though it may vary somewhat; low, limited confidence, with the estimate potentially differing from the true effect; and very low, very little confidence, with the estimate likely to differ significantly.
Two or more members of the Development Committee drafted guidelines for each PICO KQ. In this guideline, evidence-based recommendations were drafted in terms of strength and direction (strong for: the desirable effects of adherence to a recommendation outweigh the undesirable effects or weak for: the desirable effects of adherence to a recommendation probably outweigh the undesirable effects, but is not confident).8 This strength of recommendation (SOR) was determined on the basis of QOE, balance scale between desirable and undesirable effects, values and preferences, and resources (costs). The CPG was finalized after several rounds of revisions and meetings until all discrepancies were fully resolved. All CPG members reviewed the final version of the CPG document.
RESULTS
1. Evidence-based recommendations
Finally, seven KQs were selected to develop evidence-based recommendations. A total of 16 studies were suitable for the KQs (Supplementary Figure 1, available online), and the assessment of the risk of bias of each study is presented in Supplementary Figure 2 (available online).
1) Key question 1
For patients with cluster headache, is acute treatment with triptans effective?
(1) PICO elements
- Population: adult patients with CH
- Intervention: subcutaneous sumatriptan, intranasal zolmitriptan, intranasal sumatriptan, and oral zolmitriptan
- Comparator: other treatment, placebo, or no treatment
- Outcome: pain relief and freedom at 15 or 30 minutes
- Study design: double-blind randomized clinical trial
(2) Summary of evidence
Six studies were selected for answering this question (Table 1).9-14
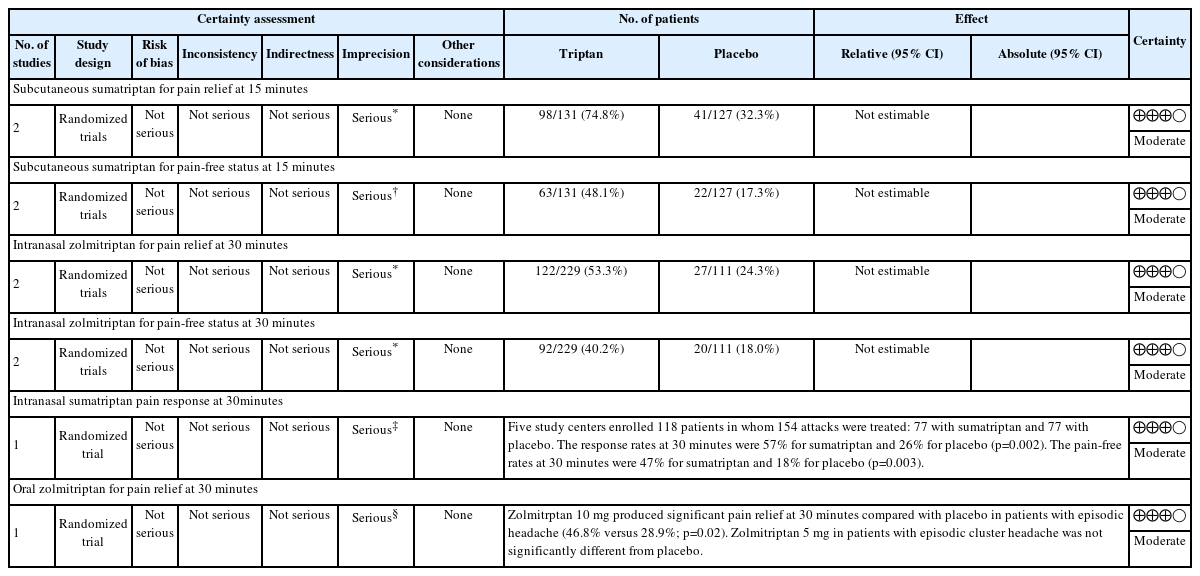
GRADE summary of findings table: subcutaneous sumatriptan, intranasal zolmitriptan, intranasal sumatriptan, and oral zolmitriptan for the acute treatment of cluster headache
① Subcutaneous sumatriptan
The efficacy of subcutaneous sumatriptan has been demonstrated in two randomized placebo-controlled trials. In a 1991 crossover study published by the Sumatriptan Cluster Headache Study Group, 49 patients were randomly assigned to receive placebo or subcutaneous sumatriptan in a random sequence, and outcomes were available for 39 patients.9 At 15 minutes after treatment of a CH attack, pain relief (pain-free or mild pain) was observed in 74% of patients treated with subcutaneous sumatriptan 6 mg compared with 26% of those receiving placebo, demonstrating the significant superiority of sumatriptan.
In another three-arm crossover trial conducted by Ekbom et al.10, a total of 157 patients were randomly assigned to receive subcutaneous sumatriptan 6 mg, sumatriptan 12 mg, or placebo in random order. At 10 minutes after administration, pain relief was observed in 25% of patients receiving placebo, 49% receiving sumatriptan 6 mg, and 63% receiving sumatriptan 12 mg. At 15 minutes, the corresponding proportions were 35%, 75%, and 80%, respectively, demonstrating that both doses of sumatriptan were significantly superior to placebo.
A Cochrane meta-analysis evaluated two randomized, placebo-controlled trials of subcutaneous sumatriptan 6 mg for the acute treatment of CH.15 Subcutaneous sumatriptan 6 mg significantly increased the likelihood of complete pain relief at 15 minutes compared with placebo (risk ratio [RR], 2.77; 95% confidence interval [CI], 1.82–4.21). Similarly, the likelihood of pain relief at 15 minutes was higher with sumatriptan (RR, 2.31; 95% CI, 1.77–3.03). The number needed to treat (NNT) for achieving pain freedom at 15 minutes was 3.3 (95% CI, 2.4–5.0). Evidence for subcutaneous sumatriptan 12 mg is limited to a single randomized controlled trial, and no pooled analysis has been performed. Regarding safety, the same Cochrane meta-analysis showed that at least one adverse event occurred in 34% of CH attacks treated with subcutaneous sumatriptan 6 mg, compared with 19% in the placebo group (relative risk, 1.8; 95% CI, 1.2–2.7). Most adverse events were mild to moderate, including injection site reactions, flushing, sweating, fatigue, warmth sensation, and pressure sensations, and did not lead to treatment discontinuation. No serious adverse events were reported.
Subcutaneous sumatriptan is more likely to abort or substantially relieve moderate-to-severe CH attacks compared with placebo. Given the low risk of serious adverse events, the balance of benefits and harms favors the use of subcutaneous sumatriptan.
② Intranasal zolmitriptan
Intranasal zolmitriptan at doses of 5 mg and 10 mg has been evaluated in two randomized placebo-controlled crossover trials. In a randomized, placebo-controlled crossover study published by Cittadini et al.11, 92 patients (59 with episodic CH and 33 with chronic CH) were randomly assigned to receive placebo, zolmitriptan nasal spray 5 mg, or 10 mg in random order for three CH attacks. At 30 minutes after treatment, pain relief (pain-free or mild pain) was observed in 62% of patients treated with zolmitriptan 10 mg and 40% of those treated with 5 mg, compared with 21% of those receiving placebo. In the subgroup analysis, the proportion of patients achieving pain relief at 30 minutes among those with episodic CH was 47% with zolmitriptan 5 mg and 80% with zolmitriptan 10 mg, whereas the corresponding proportions among patients with chronic CH were 28% and 36%, respectively, suggesting greater treatment efficacy in episodic than in chronic CH.
In another randomized placebo-controlled crossover trial conducted by Rapoport et al.12 involving 52 patients (37 with episodic CH and 15 with chronic CH), headache relief at 30 minutes was achieved in 63% of patients treated with zolmitriptan 10 mg, 50% with zolmitriptan 5 mg, and 30% with placebo.
A Cochrane meta-analysis evaluated two randomized, placebo-controlled trials of intranasal zolmitriptan (5 mg and 10 mg) for the acute treatment of CH.15 For zolmitriptan 5 mg, the likelihood of being pain-free at 15 minutes was higher than with placebo (RR, 2.60; 95% CI, 0.81–8.46), although the CI included the null. The 15-minute pain relief rate was also increased (RR, 2.20; 95% CI, 0.99–4.67). At 30 minutes, zolmitriptan 5 mg significantly improved both the pain-free rate (RR, 1.81 [95% CI, 1.12–2.90]; NNT, 6.9 [95% CI, 3.9–30]) and the pain relief rate (RR, 1.74 [95% CI, 1.20–2.51]; NNT, 5.2 [95% CI, 3.2–14]). For zolmitriptan 10 mg, the 15-minute pain-free rate was significantly higher compared with placebo (RR, 3.90 [95% CI, 1.26–12.05]; NNT, 11 [95% CI, 6.4–49]), as was the 15-minute pain relief rate (RR, 3.90 [95% CI, 1.90–8.01]; NNT, 4.9 [95% CI, 3.3–9.2]). At 30 minutes, zolmitriptan 10 mg also increased the likelihood of pain freedom (RR, 2.68 [95% CI, 1.72–4.17]; NNT, 3.3 [95% CI, 2.4–5.4]), while the improvement in pain relief did not reach statistical significance (RR, 2.36 [95% CI, 0.67–3.34]). Regarding safety, a Cochrane meta-analysis reported that at least one adverse event occurred in 27% of CH attacks treated with zolmitriptan 5 mg, compared with 15% in the placebo group (RR, 1.80 [95% CI, 1.2–2.8]). For zolmitriptan 10 mg, adverse events occurred in 37% of attacks, compared with 15% in the placebo group (RR, 2.40 [95% CI, 1.6–3.7]). The most commonly reported adverse events were taste disturbance, nausea, chest discomfort, and fatigue, and were generally mild.
Intranasal zolmitriptan is more likely to abort or substantially relieve moderate-to-severe CH attacks compared with placebo, and the risk of serious adverse events is low. Therefore, the balance of benefits and harms favors its use.
③ Intranasal sumatriptan
The efficacy of intranasal sumatriptan has been demonstrated in a 2003 randomized placebo-controlled crossover trial using a 20 mg dose.13 In this study, 118 patients (89 with episodic CH and 29 with chronic CH) were enrolled, and a total of 154 CH attacks were treated. Patients were randomly assigned to receive intranasal sumatriptan 20 mg or placebo in random order for two attacks. At 30 minutes after treatment, pain relief (pain-free or mild pain) was observed in 57% of patients treated with sumatriptan compared with 26% of those receiving placebo. Complete pain freedom at 30 minutes was achieved in 47% of patients treated with sumatriptan and 18% of those receiving placebo. Sumatriptan was also superior to placebo in relieving associated symptoms. Two patients reported chest pressure, but no serious adverse events were reported. The most frequently reported adverse event was a bitter taste, occurring in 21% of patients treated with sumatriptan and 1% of those receiving placebo.
For moderate to severe CH attacks, intranasal sumatriptan increases the likelihood of aborting or substantially relieving attacks compared with placebo, while the risk of serious adverse events is low; thus, the balance of benefits and harms favors its use.
④ Oral zolmitriptan
The efficacy of oral zolmitriptan has been demonstrated in a 2000 randomized placebo-controlled trial evaluating doses of 5 mg and 10 mg.14 In patients with episodic CH, the headache relief rate at 30 minutes was 60% with zolmitriptan 10 mg and 57% with zolmitriptan 5 mg, both of which were significantly higher than that observed with placebo (42%). Reported adverse events included paresthesia, asthenia, nausea, dizziness, and pressure sensation; however, no serious adverse events were reported.
Oral zolmitriptan is more likely to abort or substantially relieve moderate-to-severe CH attacks compared with placebo, and the risk of serious adverse events is low. Therefore, the balance of benefits and harms favors its use.
(3) Recommendation
- Subcutaneous sumatriptan is recommended for the acute treatment of CH attacks in adult patients with CH (SOR: Strong for, QOE: Moderate).
- Intranasal zolmitriptan is recommended for the acute treatment of CH attacks in adult patients with CH (SOR: Strong for, QOE: Moderate).
- Intranasal sumatriptan is recommended for the acute treatment of CH attacks in adult patients with CH (SOR: Strong for, QOE: Moderate).
- Oral zolmitriptan is recommended for the acute treatment of CH attacks in adult patients with CH (SOR: Strong for, QOE: Moderate).
2) Key question 2
For patients with cluster headache, is acute treatment with oxygen effective?
(1) PICO elements
- Population: adult patients with CH
- Intervention: oxygen
- Comparator: air placebo (room air)
- Outcome: pain relief and freedom at 15 or 30 minutes
- Study design: double-blind randomized clinical trial
(2) Summary of evidence
Two randomized placebo-controlled trials have demonstrated the effectiveness of oxygen therapy for acute CH attacks (Table 2).16,17 In a randomized crossover trial published by Fogan16 in 1985, 19 patients with CH were enrolled. For consecutive attacks in each participant, either 100% oxygen or room air was randomly administered via a non-rebreather face mask at a flow rate of 6 L/min for 15 minutes.16 Oxygen treatment showed a significant benefit compared with room air.

GRADE summary of findings table: oxygen for the acute treatment of cluster headache
In a randomized crossover trial published in 2009 by Cohen and colleagues,17 109 participants were treated with either 100% oxygen or room air delivered through a non-rebreather mask at a flow rate of 12 L/min for 15 minutes. At 15 minutes, complete pain relief or substantial improvement was reported in 78% of attacks treated with oxygen compared with 20% with room air, demonstrating a significant benefit of oxygen therapy.
Overall, high-flow oxygen delivered via a non-rebreather mask (6 or 12 L/min) increases the likelihood of complete pain relief or substantial improvement within 15 minutes compared with placebo in patients with CH attacks. As the risk of harm is very low, the balance of benefits and harms favors its use.
(3) Recommendation
Oxygen is recommended for the acute treatment of CH attacks in adult patients with CH (SOR: Strong for, QOE: Moderate).
3) Key question 3
For patients with cluster headache, is preventive treatment with suboccipital steroid injection effective?
(1) PICO elements
- Population: adult patients with CH
- Intervention: suboccipital steroid injection
- Comparator: other treatment, placebo, or no treatment
- Outcome: decrease in the frequency of attacks
- Study design: double-blind randomized clinical trial
(2) Summary of evidence
Two placebo-controlled randomized trials have demonstrated the effectiveness of suboccipital steroid injections for CH (Table 3).18,19 In a randomized study published in Italy in 2005, 23 patients with CH (16 with episodic and 7 with chronic CH) received a single injection at the ipsilateral greater occipital nerve of either a mixture of long-acting and short-acting betamethasone or placebo (2 mL of saline with 0.5 mL of lidocaine).18 At 1 week after injection, headache remission occurred in 11 of 13 patients (85%) treated with suboccipital steroids, whereas none of the 10 patients in the placebo group showed improvement (0%), demonstrating superiority over placebo.
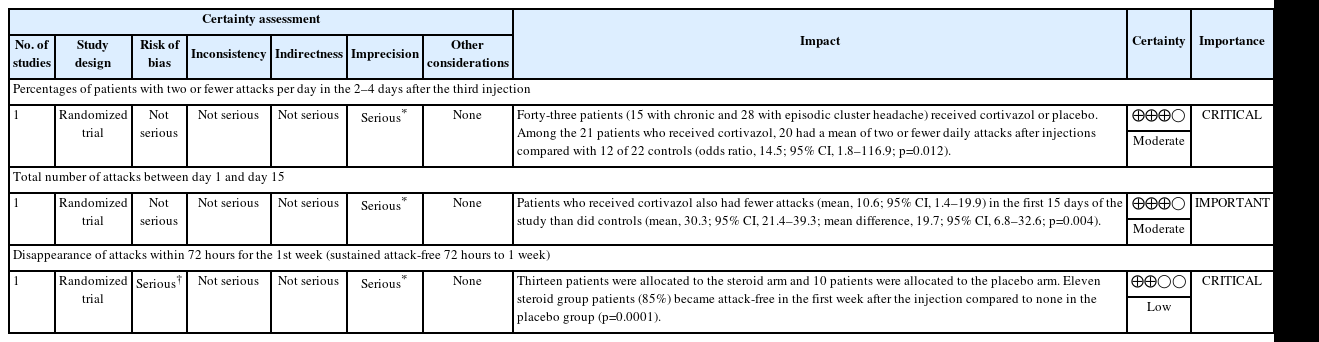
GRADE summary of findings table: suboccipital steroid injection for the preventive treatment of cluster headache
In a placebo-controlled randomized trial published in France in 2011, 43 patients with CH (28 with episodic and 15 with chronic CH) received injections of either 3.75 mg of cortivazol or the same volume of saline at the ipsilateral greater occipital nerve.19 Injections were administered three times at 48–72-hour intervals. In the cortivazol group, 95% of patients experienced a reduction in attack frequency to two or fewer attacks per day 2–4 days after the last injection, compared with 55% in the placebo group.
For the prevention of CH, suboccipital steroid injection increases the likelihood of reducing attack frequency compared with placebo. Because the risk of serious adverse events is low, the balance of benefits and harms favors treatment.
(3) Recommendation
Suboccipital steroid injection is recommended for the preventive treatment in adult patients with CH (SOR: Strong for, QOE: Moderate).
4) Key question 4
For patients with cluster headache, is preventive treatment with corticosteroids effective?
(1) PICO elements
- Population: adult patients with CH
- Intervention: corticosteroids
- Comparator: other treatment, placebo, or no treatment
- Outcome: decrease in the frequency of attacks
- Study design: double-blind randomized clinical trial
(2) Summary of evidence
One placebo-controlled randomized trial has demonstrated the effectiveness of oral corticosteroids for episodic CH (Table 4).20 In a randomized trial published in Germany in 2021, 116 patients with episodic CH were randomly assigned to a prednisone group (n=57) or a placebo group (n=59).20 Patients in the prednisone group received 100 mg of prednisone daily for 5 days, followed by tapering of 20 mg every 3 days. The primary outcome was attack frequency during the first week after initiation of the study medication. The mean number of attacks during the first week was significantly lower in the prednisone group (7.1 attacks) than in the placebo group (9.5 attacks). All participants received concomitant verapamil, which was initiated at 120 mg per day and gradually titrated to 360 mg by day 19, after which the dose was maintained. Serious adverse events occurred only in the placebo group (two cases). Adverse events reported in the prednisone group were mainly headache, palpitations, dizziness, and nausea. This study demonstrated that oral prednisone is effective as a short-term preventive treatment for episodic CH and suggested that it may be considered a first treatment option when used in conjunction with up-titration of verapamil.
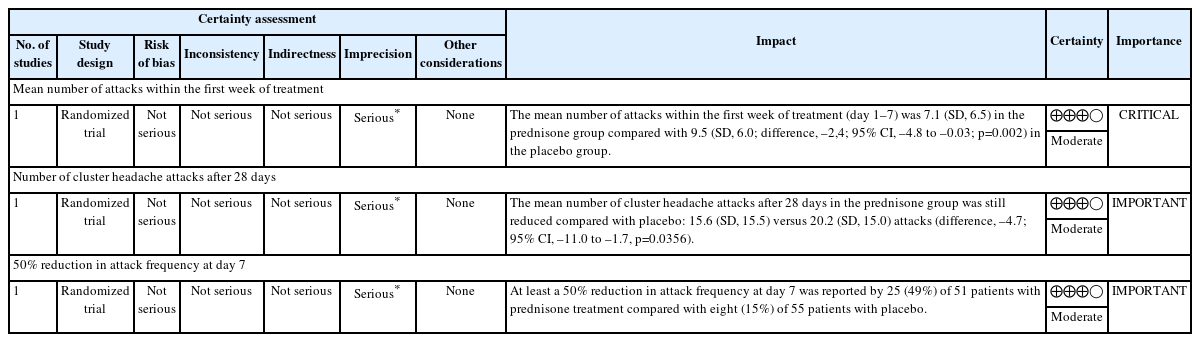
GRADE summary of findings table: oral corticosteroids for the preventive treatment of cluster headache
Overall, oral corticosteroids used during the early phase of preventive treatment are more likely than placebo to reduce attack frequency in patients with CH. As the risk of serious adverse events is low, the balance of benefits and harms favors their use.
(3) Recommendation
Oral corticosteroids are recommended for the preventive treatment in adult patients with CH (SOR: Strong for, QOE: Moderate).
5) Key question 5
For patients with cluster headache, is preventive treatment with lithium effective?
(1) PICO elements
- Population: adult patients with CH
- Intervention: lithium
- Comparator: other treatment, placebo, or no treatment
- Outcome: headache index or remission
- Study design: double-blind clinical trial
(2) Summary of evidence
Two double-blind trials have evaluated lithium for the prevention of CH, comparing lithium with placebo and with verapamil, and yielded inconsistent results (Table 5).21,22 In a multicenter double-blind crossover trial published in 1990 comparing the preventive effects of lithium and verapamil, outcome data were available for 24 patients with CH.21 Lithium and verapamil showed similar efficacy in preventing CH attacks; however, verapamil was associated with fewer adverse events and a shorter time to onset of preventive effect.
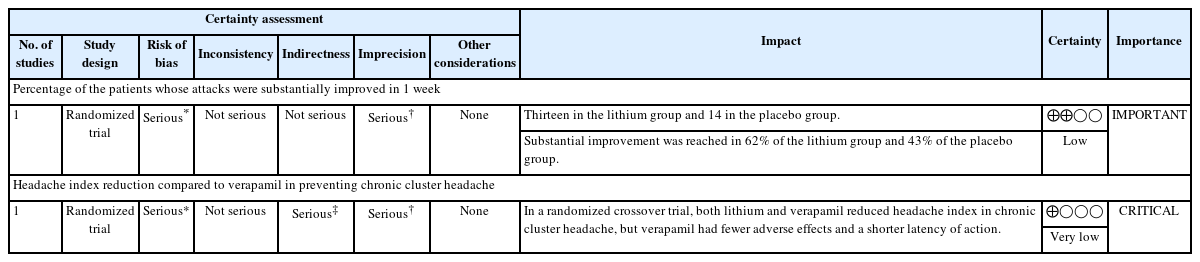
GRADE summary of findings table: lithium for the preventive treatment of cluster headache
A double-blind trial published in 1997 comparing lithium with placebo was terminated early at the interim analysis because the primary outcome was not met.22
Overall, evidence from well-designed placebo-controlled randomized trials supporting the preventive efficacy of lithium in CH is limited, and two older double-blind studies have shown inconsistent results. Nevertheless, observational studies have reported favorable outcomes, and most adverse events were mild. Therefore, lithium may be considered as a preventive treatment option for CH.
(3) Recommendation
Lithium is recommended for the preventive treatment in adult patients with CH (SOR: Weak for, QOE: Low).
6) Key question 6
For patients with cluster headache, is preventive treatment with verapamil effective?
(1) PICO elements
- Population: adult patients with CH
- Intervention: verapamil
- Comparator: other treatment, placebo, or no treatment
- Outcome: decrease in the frequency of attacks or acute medication use
- Study design: double-blind randomized clinical trial
(2) Summary of evidence
Two double-blind randomized trials have evaluated the preventive efficacy of verapamil for CH (Table 6).21,23 In a multicenter double-blind crossover trial published in 1990 comparing lithium and verapamil, outcome data were available for 24 of the 30 enrolled participants. Lithium and verapamil showed similar efficacy in preventing attacks in patients with chronic CH.21 However, verapamil was associated with fewer adverse events and a shorter time to onset of preventive effect than lithium.
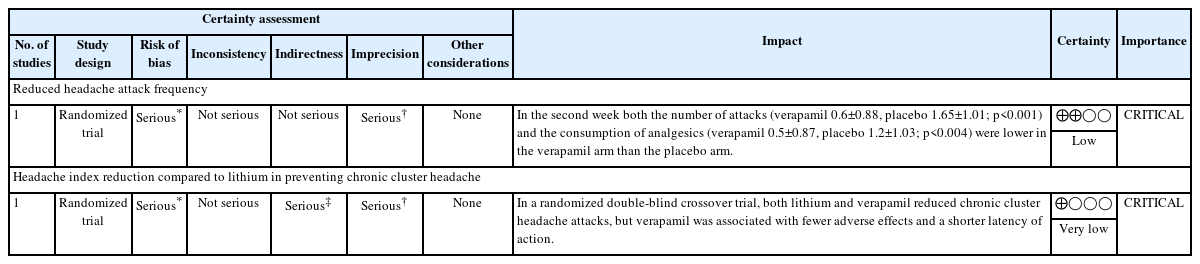
GRADE summary of findings table: verapamil for the preventive treatment of cluster headache
In a double-blind trial published in 2000 comparing verapamil with placebo in episodic CH, 30 patients were enrolled.23 Fifteen patients received verapamil 120 mg three times daily, and fifteen received placebo for 14 days. The verapamil group showed a significant reduction in attack frequency and use of acute medications compared with placebo, and only mild adverse events were reported.
Overall, despite the limited number of well-designed placebo-controlled randomized trials, verapamil has long been used in clinical practice as a preventive therapy for CH. Given its favorable safety profile and cost-effectiveness compared with other agents, the balance of benefits and harms favors its use for the prevention of CH.
(3) Recommendation
Verapamil is recommended for the preventive treatment in adult patients with CH (SOR: Strong for, QOE: Low).
7) Key question 7
For patients with cluster headache, is preventive treatment with calcitonin gene-related peptide monoclonal antibody effective?
(1) PICO elements
- Population: adult patients with CH
- Intervention: CGRP mAb
- Comparator: other treatment, placebo, or no treatment
- Outcome: decrease in the frequency of attacks
- Study design: double-blind randomized clinical trial
(2) Summary of evidence
Two placebo-controlled double-blind randomized trials have evaluated the CGRP mAb galcanezumab for the prevention of CH, one in episodic CH and the other in chronic CH (Table 7).4 In a randomized double-blind placebo-controlled trial in patients with episodic CH, subcutaneous galcanezumab 300 mg significantly reduced the weekly attack frequency compared with placebo at week 3 after treatment initiation.4
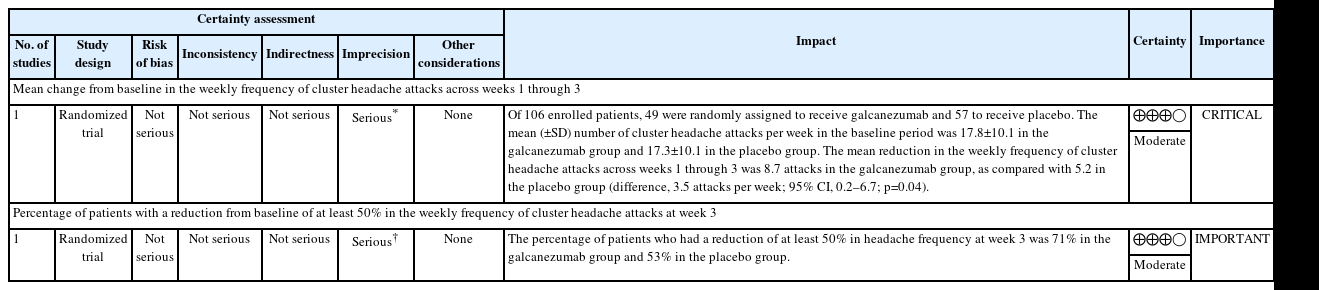
GRADE summary of findings table: galcanezumab for the preventive treatment of episodic cluster headache
However, in another placebo-controlled double-blind randomized trial conducted in patients with chronic CH, galcanezumab did not show a significant reduction in attack frequency compared with placebo.24
In Korea, real-world evidence on the preventive efficacy of galcanezumab 240 mg for CH has also been reported.25 In a multicenter observational study conducted at three institutions, 50 patients with CH received at least one dose of galcanezumab 240 mg either as monotherapy or in combination with standard therapy. Among the 47 patients with episodic CH included in the analysis, the median time to complete remission after treatment was 17 days. The cumulative complete remission rates were 28% within 1 week, 49% within 2 weeks, and 62% within 3 weeks.
Overall, treatment with galcanezumab in patients with episodic CH significantly reduces attack occurrence, and the risk of adverse events appears to be very low. Therefore, the balance of benefits and harms favors its use as a preventive treatment for episodic CH.
(3) Recommendation
Galcanezumab is recommended for the preventive treatment in adult patients with episodic CH (SOR: Strong for, QOE: Moderate).
2. Expert consensus
1) Other acute treatment
(1) Other triptans
① Summary of evidence
The efficacy of several triptan formulations for the acute treatment of CH has been demonstrated, including intranasal sumatriptan, subcutaneous sumatriptan, oral zolmitriptan, and intranasal zolmitriptan. However, the efficacy of other triptans and formulations has not been established in randomized controlled trials. In Korea, the use of subcutaneous or intranasal triptans is currently not available; therefore, oral zolmitriptan is the only triptan formulation commonly used in clinical practice. In patients who do not respond to or cannot tolerate oral zolmitriptan, alternative treatment options are needed.
Two observational studies have reported the effectiveness of oral triptans other than zolmitriptan for the acute treatment of CH. In a prospective multicenter observational study conducted in Korea evaluating the effectiveness of various acute treatments, 155 of 262 patients with CH (249 with episodic and 13 with chronic CH) used different oral triptans, and 140 of these patients (90.3%) reported a beneficial effect.26 In addition, an internet-based international patient satisfaction survey conducted in more than 50 countries included 2,193 patients, including 1,604 with CH and 589 with probable CH. In this survey, 54% of respondents reported that triptans were completely or very effective for the acute treatment of CH.27
Triptans differ in their pharmacokinetic properties depending on the specific agent and formulation, but they exert their therapeutic effect in the acute treatment of CH primarily through selective agonism of the 5-HT1B and 5-HT1D serotonin receptors. Therefore, if triptans recommended based on evidence cannot be used or are ineffective, treatment with alternative triptans may be considered. However, because triptans cause vasoconstriction, they may be associated with cardiovascular or cerebrovascular adverse events and are contraindicated in patients with underlying cardiovascular or cerebrovascular disease.
② Recommendation
Oral triptans, including sumatriptan, almotriptan, naratriptan, and frovatriptan are recommended for the acute treatment of adult patients with CH when evidence-based acute treatments are unavailable or ineffective (Expert consensus).
(2) Non-steroidal anti-inflammatory drugs and ergot derivatives
① Summary of evidence
No well-designed double-blind randomized placebo-controlled trials have evaluated the efficacy of non-steroidal anti-inflammatory drugs (NSAIDs) or combination analgesics for the acute treatment of CH. However, evidence from a prospective multicenter observational study conducted in Korea has reported their potential treatment effects.26 Among 262 patients (249 with episodic CH and 13 with chronic CH), 71 of 86 patients (82.6%) who used NSAIDs and nine of 12 patients (75.0%) who used combination analgesics reported treatment benefit. In particular, among patients who used NSAIDs as monotherapy, nine of 15 patients (60.0%) reported treatment benefit, whereas 61 of 71 patients (85.9%) reported benefit when NSAIDs were used in combination with other medications.
A small double-blind placebo-controlled crossover trial evaluated the efficacy of intranasal dihydroergotamine for the acute treatment of CH.28 In this study involving 25 patients, intranasal dihydroergotamine reduced headache intensity compared with placebo, but did not improve attack frequency or duration.
② Recommendation
In adult patients with CH, NSAIDs are recommended as adjunctive therapy, or ergot derivatives are recommended when evidence-based acute treatments are unavailable, contraindicated, or insufficiently effective (Expert consensus).
(3) Octreotide
① Summary of evidence
One double-blind, placebo-controlled crossover trial evaluated the efficacy of subcutaneous octreotide for the acute treatment of CH.29 In this study, patients experiencing moderate to severe CH attacks received 100 μg of octreotide administered subcutaneously or placebo. Among a total of 57 patients, efficacy data were available for 46 attacks in the octreotide group and 45 attacks in the placebo group. Treatment response was assessed 30 minutes after injection, and a response was observed in 52% of attacks treated with octreotide compared with 36% of attacks treated with placebo. No serious adverse events were reported. However, 17% of patients receiving octreotide experienced adverse effects, including gastrointestinal discomfort, dizziness, and diarrhea, whereas 9% of patients in the placebo group reported adverse effects. In addition to only mild gastrointestinal symptoms, octreotide does not cause vasoconstriction, which may represent a potential safety advantage in patients in whom vasoconstrictive agents are contraindicated.
② Recommendation
In adult patients with CH, subcutaneous octreotide is recommended when evidence-based acute treatments are unavailable, contraindicated, or insufficiently effective (Expert consensus).
(4) Lidocaine
① Summary of evidence
There are no well-designed randomized double-blind trials evaluating the efficacy of intranasal lidocaine for the acute treatment of CH. However, several small studies have investigated its potential benefit.
One small double-blind, placebo-controlled study evaluated the effect of intranasal lidocaine in patients with CH in whom attacks were induced by sublingual nitroglycerin (0.9 mg).30 A total of 15 patients with CH participated in the study, and headache attacks were successfully induced in nine patients. These patients received intranasal cocaine or 10% lidocaine spray. Compared with placebo (saline), intranasal lidocaine significantly reduced pain intensity, and the mean time to complete pain relief was 37.0±7.8 minutes in the lidocaine group versus 59.3±7.8 minutes in the saline group (p<0.05).
Another randomized double-blind study conducted in an emergency department evaluated intranasal lidocaine in patients presenting with primary headache disorders, including CH.31 Patients were randomly assigned to receive 2% intranasal lidocaine or saline placebo. Among 100 patients, 50 were assigned to each group, and CH accounted for 46% of patients in the lidocaine group and 20% in the placebo group. At 30 minutes after treatment, pain intensity reduction and treatment success rates were significantly greater in the lidocaine group.
In addition, an observational study involving 30 male patients with CH evaluated 4% intranasal lidocaine and reported moderate pain relief in 27% of patients.32
Because shock has been reported following administration of lidocaine, patients are advised to remain at rest in bed for approximately 20–30 minutes after administration.33 In addition, adverse effects are relatively common compared with its therapeutic benefit, and therefore caution should be exercised when using this medication.
② Recommendation
In adult patients with CH, intranasal lidocaine is recommended when evidence-based acute treatments are unavailable, contraindicated, or insufficiently effective (Expert consensus).
2) Other preventive treatment
(1) Topiramate
① Summary of evidence
Two open-label studies have evaluated the preventive efficacy of topiramate in patients with CH.
In an open-label clinical study conducted in Taiwan, the preventive effect of topiramate was assessed in 13 patients with CH (12 with episodic CH and 1 with chronic CH).34 Treatment results showed that 10 patients (9 with episodic CH and 1 with chronic CH) experienced a reduction in the duration of the cluster period to approximately half of the previous duration, suggesting a potential preventive effect of topiramate.
Another open-label study conducted in the United States evaluated 26 patients with episodic CH and 10 patients with chronic CH, all diagnosed according to the International Classification of Headache Disorders criteria.35 Patients were treated with topiramate for 20 days after the first 7 days of headache attacks. Among the 33 patients who completed the study, 21% experienced a ≥50% reduction in daily headache frequency.
The main adverse events associated with topiramate included paresthesia, slow speech, and dizziness in the Taiwanese study,34 and paresthesia, visual discomfort, confusion, and hypersomnia in the U.S. study.35
② Recommendation
In adult patients with CH, topiramate is recommended when evidence-based preventive treatments are unavailable, contraindicated, or insufficiently effective (Expert consensus).
(2) Valproic acid
① Summary of evidence
The preventive efficacy of valproic acid in CH has been evaluated in both open-label and randomized placebo-controlled studies, with inconsistent results.
In a small open-label study involving 15 patients with CH (13 with episodic and 2 with chronic CH), 11 patients responded to treatment with valproic acid (600–1,200 mg/day).36 Among these, nine patients achieved complete remission and two patients showed partial remission. Adverse events were minimal, with only mild nausea reported in three patients.
In contrast, a randomized placebo-controlled trial including 96 patients with CH found no significant differences between the valproic acid and placebo groups in terms of headache-free days, attack frequency, intensity, or duration.37 Moreover, adverse events were more frequent in the valproic acid group than in the placebo group, with nausea, vomiting, and somnolence being the most common.
Overall, the available evidence is insufficient to support the use of valproic acid as a primary preventive treatment for CH. However, valproate may be considered in patients who have an inadequate response to, or cannot tolerate, established preventive therapies.
The onset of preventive efficacy of valproic acid in CH has not been well established; however, it should be noted that clinical benefit may take at least 4 weeks to become apparent.
② Recommendation
In adult patients with CH, valproic acid is recommended when evidence-based preventive treatments are unavailable, contraindicated, or insufficiently effective (Expert consensus).
(3) Melatonin
① Summary of evidence
The evidence supporting the preventive efficacy of melatonin in CH is limited, and no large well-designed randomized placebo-controlled trials are available. Only a small number of pilot studies have been reported, with inconsistent findings.
In a double-blind, placebo-controlled pilot study with a parallel-group design, 20 patients with CH were randomized to receive melatonin 10 mg (n=10) or placebo (n=10) for 14 days.38 The melatonin group showed a significant reduction in headache frequency (p<0.03) and a trend toward reduced analgesic use (p<0.06) compared with placebo.
In a subsequent pilot study evaluating melatonin as add-on therapy in patients who did not achieve complete remission with primary preventive treatments, both chronic and episodic CH patients were included.39 Patients received melatonin and placebo in a sequential manner over one-month periods. Outcomes included daily headache frequency, analgesic use, and headache severity (mild, moderate, severe). There were no significant differences between the melatonin and placebo groups across these outcomes.
Overall, melatonin may be considered as an alternative preventive option in patients with CH who have an inadequate response to or failure of established preventive treatments.
In addition, melatonin is generally well tolerated with a favorable safety profile compared with other preventive agents. Given that sleep disturbances are common in patients with CH, melatonin may be particularly considered in patients with coexisting sleep disorders.
② Recommendation
In adult patients with CH, melatonin is recommended when evidence-based preventive treatments are unavailable, contraindicated, or insufficiently effective (Expert consensus).
3) Neuromodulation
(1) Non-invasive vagus nerve stimulation
① Summary of evidence
The efficacy of non-invasive vagus nerve stimulation (nVNS) for CH has been evaluated in both acute and preventive settings, including two randomized controlled trials and one meta-analysis for acute treatment, and one randomized open-label trial for prevention.
For acute treatment, two randomized, double-blind, sham-controlled trials (ACT1 and ACT2) have been reported.40,41 In the ACT1 trial including 133 patients with CH, the response rate was 26.7% in the nVNS group and 15.1% in the sham group, with no statistically significant difference (p=0.1). In the ACT2 trial involving 92 patients, the 15-minute response rates were 14% in the nVNS group and 12% in the sham group, also showing no significant difference (p=0.71). A subsequent meta-analysis demonstrated findings consistent with these individual trials.42 However, subgroup analyses limited to patients with episodic CH suggested that nVNS may be effective for acute treatment in this population.
For preventive treatment, one randomized open-label trial evaluated nVNS in patients with chronic CH. In this study, 45 patients received nVNS in addition to standard preventive therapy, while 48 patients received standard preventive therapy alone.43 At weeks 3–4, the group receiving nVNS showed a greater reduction in weekly attack frequency by 3.9 attacks compared with the control group (p=0.02).
nVNS is generally considered a safe treatment option for patients with CH. However, its safety has not been established in patients with significant cardiac arrhythmias, such as second- or third-degree atrioventricular block, or in those with implantable devices, including pacemakers or cochlear implants.
② Recommendation
nVNS is recommended for the acute treatment in adult patients with episodic CH (Expert consensus).
In adult patients with chronic CH, nVNS is recommended as adjunctive therapy to evidence-based preventive treatments (Expert consensus).
(2) Sphenopalatine ganglion stimulation
① Summary of evidence
The efficacy of sphenopalatine ganglion (SPG) stimulation has been evaluated in patients with CH in both acute and preventive settings, including sham-controlled studies, a randomized double-blind sham-controlled trial, and open-label studies.
In a small randomized sham-controlled study involving patients with refractory chronic CH (n=32), 28 patients completed the study.44 Among them, 43% achieved a ≥50% reduction in attack frequency, and 25% experienced pain relief in ≥50% of treated attacks, indicating both preventive and acute treatment effects. In a subsequent 24-month open-label study, 45% of patients achieved an acute treatment response (pain relief in ≥50% of attacks), and 35% achieved a ≥50% reduction in attack frequency, with 61% of patients overall demonstrating a treatment response.45
Another open-label European study including 85 patients (78 with chronic and 7 with episodic CH) reported that 55% of patients with refractory chronic CH achieved a ≥50% reduction in attack frequency, and 32% achieved an acute response, resulting in an overall response rate of 67%.46
The only randomized double-blind sham-controlled trial, conducted across 21 headache centers in the United States, included 93 patients with chronic CH. Patients were randomized to active stimulation (n=45) or sham stimulation (n=48).47 At 15 minutes after treatment, pain relief was achieved in 62.4% of attacks in the active group compared with 38.8% in the sham group, demonstrating a significant benefit of SPG stimulation for acute treatment.
SPG stimulation may be considered as a treatment option for patients with refractory chronic CH who have an inadequate response to pharmacological therapies. It has the advantage of demonstrating efficacy in both acute and preventive treatment settings. However, due to its invasive nature, high cost, and variability in treatment response, SPG stimulation should be selectively considered in patients with significant disability who have failed conventional non-invasive treatment options.48
② Recommendation
SPG stimulation is recommended for both acute and preventive treatment in adult patients with refractory chronic CH (Expert consensus).
(3) Occipital nerve stimulation
① Summary of evidence
There are currently no well-designed randomized, double-blind, sham-controlled trials evaluating the efficacy of occipital nerve stimulation (ONS) compared with sham stimulation in patients with CH. Most available evidence is limited to observational studies and uncontrolled trials.
In a single-center open-label study involving 35 patients with refractory chronic CH, 66.7% of patients achieved a ≥50% reduction in daily headache frequency.49
In another cohort study of 51 patients with refractory chronic CH, 52.9% were classified as responders.50
A multicenter randomized double-blind study including 131 patients with refractory chronic CH evaluated treatment effects using 100% versus 30% stimulation intensity. In the 100% stimulation group, the mean weekly attack frequency decreased from 17.58 to 9.5, while in the 30% stimulation group it decreased from 15 to 6.75, suggesting a treatment effect in both groups.51
Overall, despite the proven efficacy for refractory CH, adverse events following ONS are relatively common, most frequently including battery depletion, lead migration, and device malfunction. However, serious adverse events are less frequent compared with deep brain stimulation (DBS), suggesting that ONS may be considered before DBS as a less invasive neuromodulation option.
② Recommendation
ONS is recommended for the preventive treatment in adult patients with refractory chronic CH (Expert consensus).
(4) Deep brain stimulation
① Summary of evidence
There is one randomized, double-blind, sham-controlled trial evaluating the efficacy of DBS in patients with CH, while most other available studies are prospective or retrospective observational studies. In many of these studies, statistical comparisons between pre- and post-treatment outcomes were not formally performed and results were primarily descriptively reported.
In the randomized double-blind sham-controlled trial including 11 patients with refractory chronic CH, no significant treatment effect was observed during the randomized phase.52 However, after a 10-month open-label extension period, 6 patients achieved a ≥50% reduction in headache frequency. To date, no well-designed follow-up randomized sham-controlled trials have been conducted.
In a meta-analysis including 40 patients with refractory chronic CH treated with DBS and followed for a mean of 44 months, the average reduction in attack frequency was 77%.53 Moreover, in another systematic review and meta-analysis published after the literature search, among 108 chronic CH patients treated with DBS, 70.1% reported a reduction in headache frequency over a mean follow-up of 45.4 months.54 Major complications occurred in 16.6% of patients and included lead damage or displacement, subcutaneous infection, neurological deficits, contralateral CH attacks, and intracerebral hemorrhage. One patient who developed intracerebral hemorrhage subsequently died.
There is currently no established consensus on the optimal target or stimulation approach for DBS, and the risk of adverse effects should be carefully weighed when considering this treatment.
② Recommendation
DBS is recommended for the preventive treatment in adult patients with refractory chronic CH (Expert consensus).
This CPG provides an evidence-based and expert-informed framework for the acute and preventive treatment of CH (Figure 1). Despite advances in the understanding and management of CH, a substantial proportion of patients remain undertreated or experience inadequate responses to currently available therapies. The authors recommend that treatment decisions should be individualized based on clinical characteristics, treatment response, comorbidities, and patient preferences. This guideline aims to support clinicians in optimizing the management of CH and improving patient outcomes in real-world clinical practice.
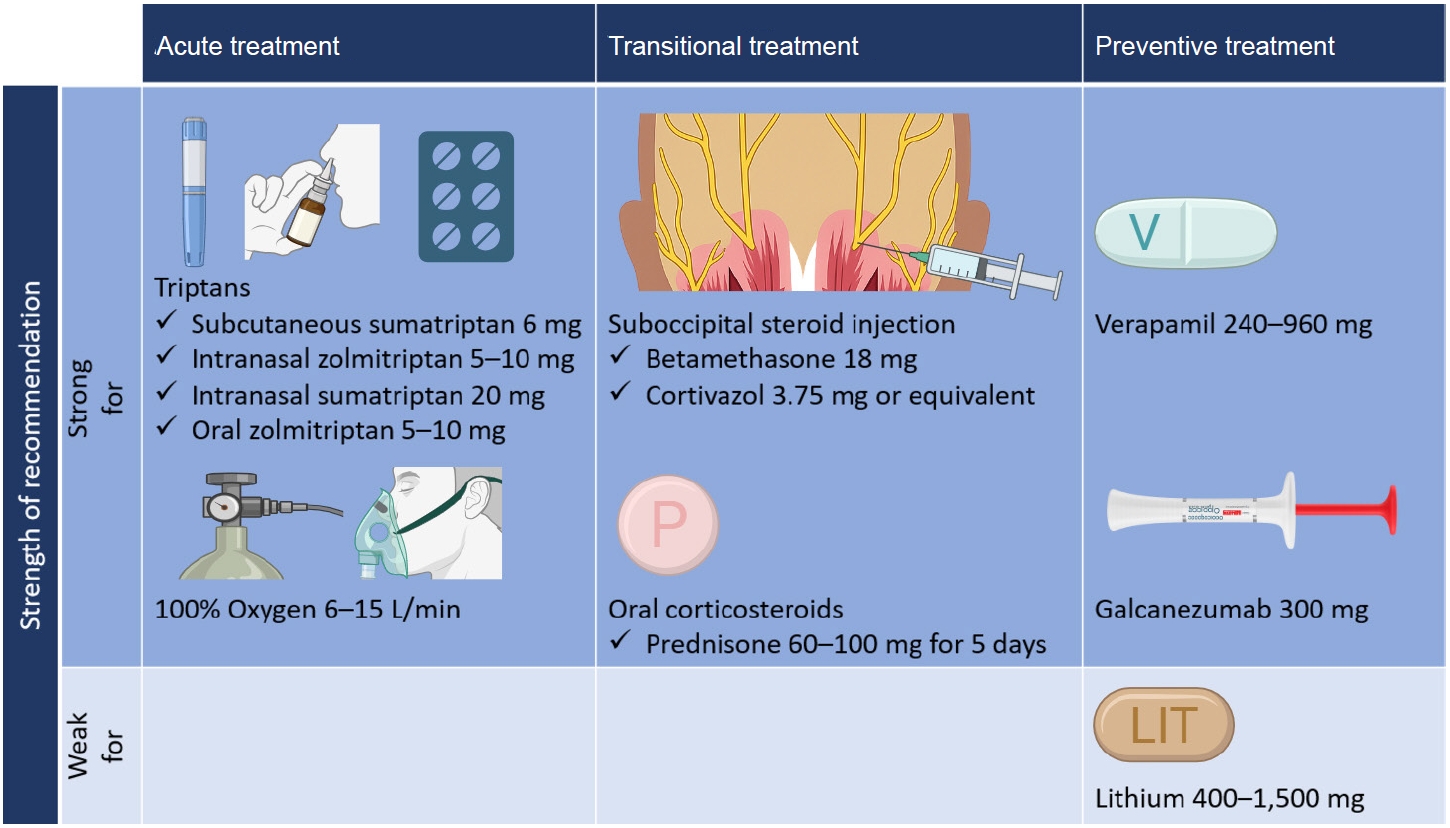
Summary of evidence-based recommendations for the treatment of cluster headache. Given the rapid onset of preventive effects and short-term benefits of suboccipital steroid injection and oral corticosteroids, these treatments are classified as transitional treatments (short-term therapies used to bridge the period until preventive treatments become effective). Created with BioRender.com.
Notes
AVAILABILITY OF DATA AND MATERIAL
Not applicable.
AUTHOR CONTRIBUTIONS
Conceptualization: BSK, PWC, HKP, MJL, JMC, MC; Data curation: BSK, PWC, HKP, MJL, JMC, MC; Formal analysis: BSK, PWC, HKP, MJL, JMC, MC; Investigation: BSK, PWC, HKP, MJL, JMC, KMK, JK, HSM, DWB, JHS, TJS, WL, SC, MJC, YJC; Methodology: BSK, PWC, HKP, MJL, JMC, MC; Supervision: BSK, PWC, HKP, MJL, JMC, MC; Writing–original draft: BSK, PWC, HKP, MJL, JMC, KMK, JK, HSM, DWB, JHS, TJS, WL, SC, MJC, YJC; Writing–review & editing: BSK, PWC, HKP, MJL, JMC, MC.
CONFLICT OF INTEREST
Mi Ji Lee is the Associate Editor of Headache and Pain Research and was not involved in the review process of this article. All authors have no other conflicts of interest to declare.
FUNDING STATEMENT
None.
ACKNOWLEDGMENTS
None.
SUPPLEMENTARY MATERIAL
Supplementary materials are available from https://doi.org/10.62087/hpr.2026.0011.
Search query
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart on the study selection process. RCT, randomized controlled trial.
Summary of assessment of risk of bias.