Abstract
-
Purpose
- Dizziness frequently coexists with headache in children and adolescents, but its diagnostic significance is often underrecognized. Orthostatic intolerance (OI) and otologic diseases are major causes of pediatric dizziness, yet distinguishing among these conditions remains clinically challenging. This study examined the diagnostic distribution of OI and otologic diseases in pediatric patients with primary headache-associated dizziness.
-
Methods
- We retrospectively reviewed 310 patients aged 7–18 years who presented with both headache and dizziness; patients with secondary headache disorders were excluded. OI was assessed using head-up tilt testing and was classified primarily as orthostatic hypotension (OH) or postural orthostatic tachycardia syndrome (POTS). Otologic diseases, mainly peripheral vestibular disorders, were identified by otolaryngologists. Statistical analyses included the chi-squared test and one-way analysis of variance.
-
Results
- The most common headache subtypes were migraine without aura (42.9%), vestibular migraine (15.8%), and tension-type headache (15.2%). OI was identified in 63.9% of patients, including OH in 40.6% and POTS in 23.2%; otologic diseases were present in 20.0%. The distributions of OI and otologic diseases did not differ significantly by headache subtype. OI was significantly associated with age and sex, with the POTS group having the highest mean age and a marked female predominance. Age also differed significantly across otologic disease subtypes.
-
Conclusion
- In pediatric patients with headache and dizziness, OI and otologic diseases were common but were not associated with headache subtype. Instead, diagnostic patterns were more closely related to age and sex, suggesting that developmental and demographic factors should be considered when evaluating headache-associated dizziness in this population.
-
Keywords: Dizziness, Headache, Orthostatic intolerance, Pediatrics, Vestibular diseases
INTRODUCTION
Headache is one of the most common neurological complaints among school-aged children in South Korea, affecting approximately 29.1% of this population.1 Dizziness is also a frequent symptom in children and adolescents and is commonly accompanied by headaches. The term dizziness encompasses a broad range of sensations, including vertigo, lightheadedness, imbalance, and presyncope. Among these, vertigo specifically refers to an illusory sensation of movement, typically a spinning sensation, and is more commonly associated with vestibular disorders.2 In pediatric patients, dizziness can arise from a wide range of etiologies, including autonomic, otologic, and neurologic conditions, reflecting the involvement of multiple physiological systems, such as the vestibular, cardiovascular, and central nervous systems, making clinical evaluation challenging.3 In addition, pediatric patients often have difficulty accurately describing their symptoms, which further complicates diagnostic assessment.4 In particular, dizziness is increasingly recognized as an important comorbidity in pediatric patients with headache, especially those with migraine, for which orthostatic intolerance (OI) and autonomic dysregulation are thought to play contributing roles.5,6
Among these etiologies, OI and otologic diseases are the most clinically relevant categories. OI, including orthostatic hypotension (OH) and postural orthostatic tachycardia syndrome (POTS), reflects an abnormal cardiovascular response to postural changes and is commonly observed in adolescents, often in association with headaches and other neurological symptoms.6,7 In contrast, otologic diseases are primarily related to peripheral vestibular dysfunction, and include conditions such as Ménière’s disease, benign paroxysmal positional vertigo (BPPV), and benign paroxysmal vertigo of childhood (BPVC), which are major causes of recurrent dizziness in the pediatric populations.3,8 Given the distinct pathophysiological mechanisms and clinical implications, distinguishing between these categories is important for evaluating pediatric dizziness.
Nevertheless, most existing studies have focused on patients presenting primarily with dizziness, rather than headache-associated dizziness.3 Consequently, the diagnostic distribution and clinical characteristics of orthostatic and otologic conditions in pediatric patients with primary headache currently remain poorly defined. In particular, whether these conditions differ according to headache subtype or are more closely related to demographic factors, such as age and sex, remains unclear.
The present study therefore aimed to investigate the frequency and diagnostic distribution of OI and otologic diseases in pediatric patients presenting with primary headache-associated dizziness in a clinical setting.
MATERIALS AND METHODS
1. Study design and participants
We conducted a retrospective review of 310 pediatric patients who visited the pediatric headache clinic at Hallym University Kangnam Sacred Heart Hospital (HUKSHH) between January 2016 and December 2021. Patients aged 7–18 years who presented with headache and dizziness were included; all patients were diagnosed with primary headache according to the third edition of the International Classification of Headache Disorders (ICHD-3) criteria.9 Vestibular migraine (vM) was analyzed as a distinct working diagnostic category for the purposes of this study. Further subclassification according to the underlying migraine subtype (migraine with or without aura) was not performed. Patients with secondary headache disorders, including structural or inflammatory central nervous system diseases, were excluded.
This study was approved by the Institutional Review Board of HUKSHH (2026-02-001). The requirement for informed consent was waived owing to the retrospective nature of the study.
2. Clinical assessment
Baseline data included demographic characteristics, medical history, and headache-related information, such as headache frequency, duration, and clinical features. Information on dizziness was also collected, including symptom characteristics, such as duration, frequency, and associated features. The head-up tilt testing (HUTT) was performed to evaluate OI when clinically indicated, particularly in patients with symptoms suggestive of autonomic dysfunction, including orthostatic dizziness, syncope, presyncope, or symptom aggravation related to postural changes. Otologic evaluation was conducted based on clinical examination and diagnostic assessment by otolaryngologists, when indicated. Imaging studies, such as brain magnetic resonance imaging, were performed as required.
3. Definitions
OI was classified as OH or POTS based on the HUTT findings10. OH was defined as a sustained reduction in systolic blood pressure of ≥20 mmHg or diastolic blood pressure of ≥10 mmHg within 3 minutes of head-up tilt, while POTS was defined as a heart rate increment of ≥40 beats per minute within 10 minutes of head-up tilt, in the absence of OH. Otologic diseases, including Ménière’s disease, BPPV, BPVC, and vestibular neuritis, were identified based on clinical diagnoses by otolaryngology specialists. Final diagnostic classification was based on the integrated clinical assessment of headache specialists and otolaryngologists using clinical information, including symptom characteristics, associated auditory features, vestibular findings, and follow-up evaluations when available.
4. Statistical analysis
Descriptive statistics were used to summarize the patient characteristics. Categorical variables were compared using the chi-squared test. When the expected cell counts were less than 5, Fisher’s exact test was used, with Monte Carlo simulations applied as appropriate. Continuous variables were compared using a one-way analysis of variance. Statistical significance was set at p-value <0.05. All statistical analyses were performed using the R software (version 4.6.0; R Foundation for Statistical Computing).
RESULTS
1. Baseline characteristics
This study included 310 pediatric patients, including 113 males (36.5%) and 197 females (63.5%), with a mean age of 12.2±2.8 years. Migraine without aura (MwoA) was the most common headache subtype, occurring in 133 patients (42.9%), followed by vM in 49 (15.8%), tension-type headache (TTH) in 47 (15.2%), other headache disorders in 46 (14.8%), and migraine with aura (MwA) in 35 (11.3%) (Table 1). A higher proportion of females was observed in the MwA (26/35, 74.3%) and vM (35/49, 71.4%) groups; however, the sex distribution did not differ significantly according to headache subtype (p=0.285).
OI was identified in 198 patients (63.9%). Among them, OH was observed in 126 (40.6%) and POTS in 72 (23.2%). The remaining 112 patients (36.1%) showed no evidence of OI. Otologic diseases were identified in 62 patients (20.0%). The most common subtype was Ménière’s disease (n=18; 5.8%), followed by vestibular neuritis (n=16; 5.2%), BPPV (n=10; 3.2%), BPVC (n=9; 2.9%), and other otologic disorders (n=9; 2.9%).
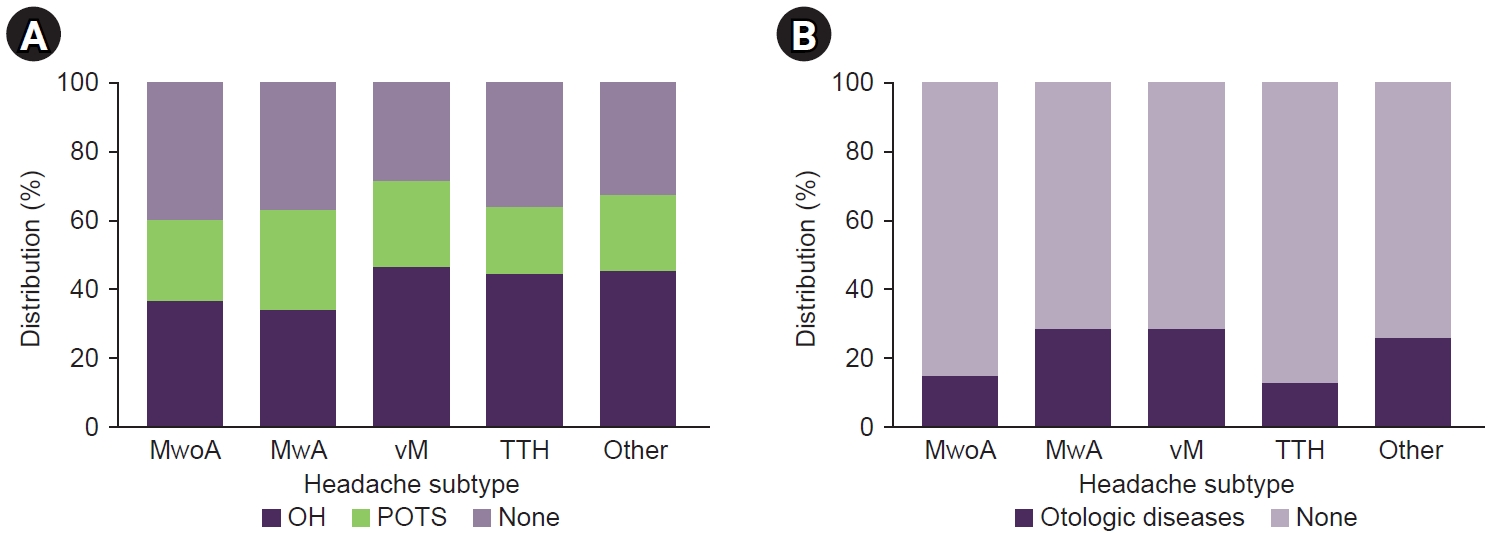
2. Association between headache subtype and orthostatic intolerance or otologic diseases
The distribution of OI (OH, POTS, and none) did not differ significantly according to headache subtype (p=0.851) (Figure 1), nor did the proportion of OH (p=0.561). The proportion of otologic diseases did not differ significantly according to the headache subtype (p=0.075) (Figure 1), although it was higher in the vM (14/49, 28.6%) and MwA (10/35, 28.6%) groups.
3. Sex differences in orthostatic intolerance
The OI categories were significantly associated with sex (p=0.005). Female predominance was particularly marked in the POTS group (57/72, 79.2%) compared to the OH group (77/126, 61.1%) and patients without OI (63/112, 56.3%).
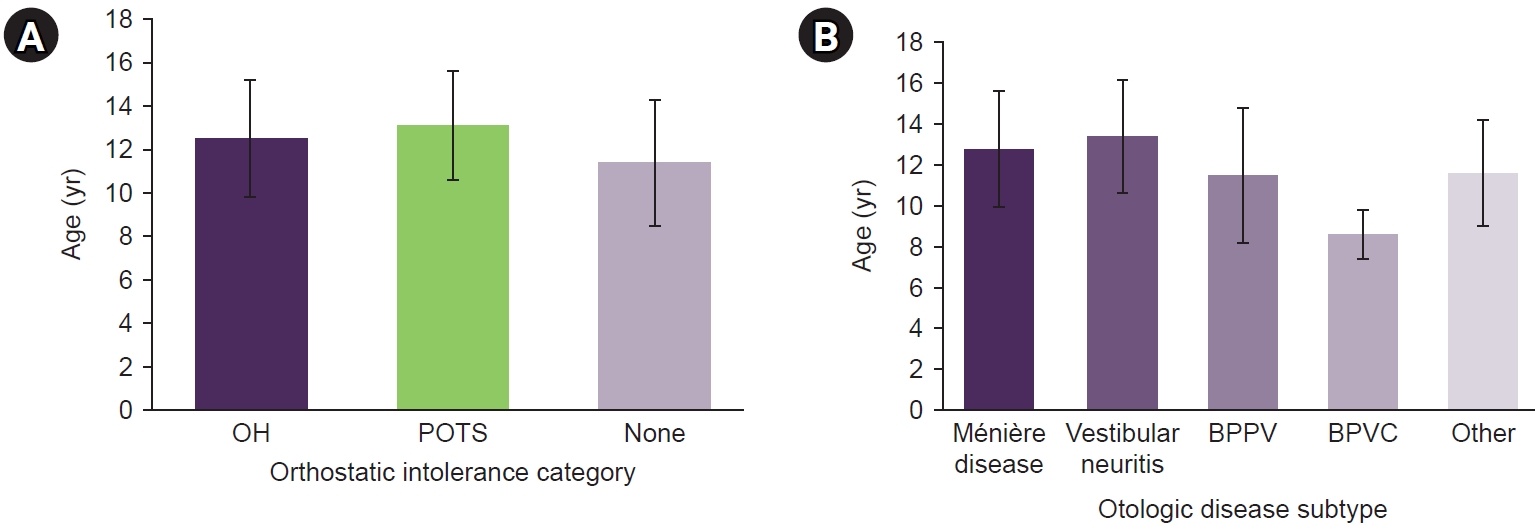
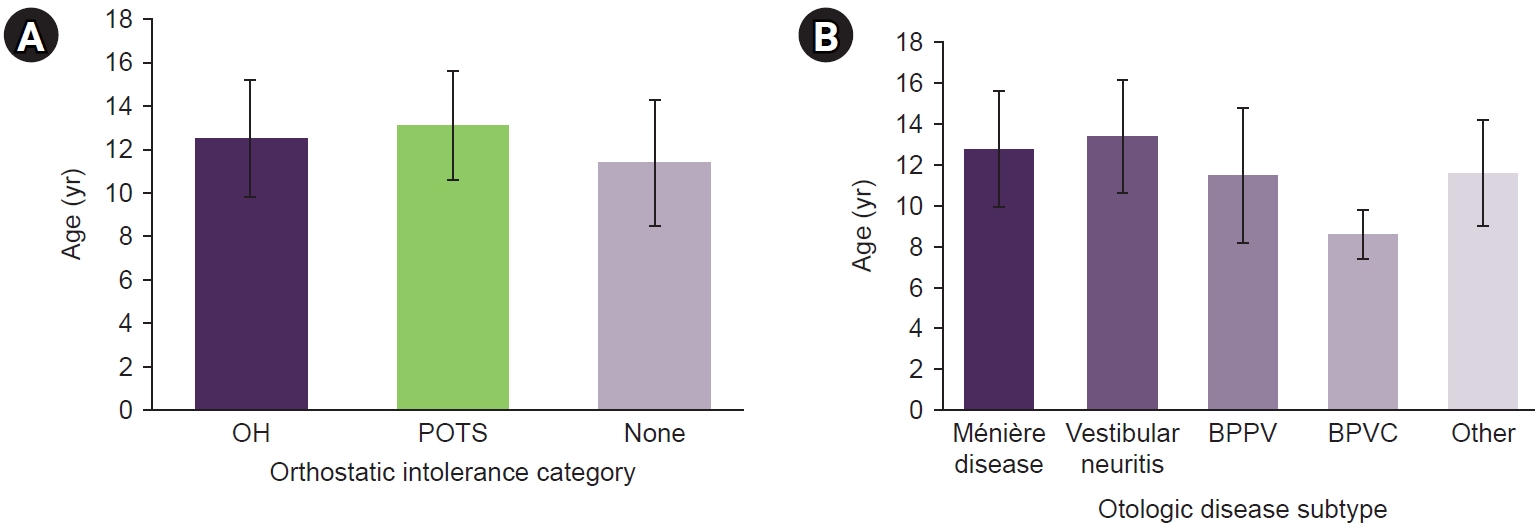
4. Age distribution according to orthostatic intolerance status and otologic diagnoses
Age differed significantly according to OI categories (p<0.001) (Figure 2), with the highest mean age observed in the POTS group (13.1±2.5 years), followed by the OH group (12.5±2.7 years), with the lowest in patients without OI (11.4±2.9 years). Post-hoc analysis showed that patients with OH and POTS were significantly older than those without OI (p=0.003 and p<0.001, respectively), whereas no significant age difference was observed between the OH and POTS groups (p=0.311). Age also differed significantly across otologic disease subtypes (p=0.003) (Figure 2); specifically, the mean age was lowest in patients with BPVC (8.6±1.2 years) and highest in those with vestibular neuritis (13.4±2.8 years). Post-hoc analysis demonstrated that patients with BPVC were significantly younger than those with Ménière’s disease (p=0.003) and vestibular neuritis (p<0.001).
5. Combined clinical phenotypes
Patients were categorized according to their combined clinical features as follows: headache alone in 91 patients (29.4%), headache with OI in 157 (50.6%), headache with otologic diseases in 21 (6.8%), and all three conditions in 41 (13.2%). The distribution of these combined clinical phenotypes did not differ significantly according to headache subtype (p=0.256).
DISCUSSION
In this study, OI was frequently observed in pediatric patients presenting with primary headache and dizziness; however, its distribution did not differ significantly according to headache subtype. In contrast, significant differences in age and sex were identified, indicating that the clinical characteristics of dizziness in pediatric headache may be influenced more by developmental and demographic factors than by headache subtype. These findings highlight the overlapping clinical features of pediatric headaches and dizziness in relation to OI.
The lack of any significant association between headache subtype and OI suggests that these conditions may reflect shared pathophysiological mechanisms across different headache subtypes, rather than any subtype-specific feature. Prior studies have demonstrated that migraine and OI commonly coexist in pediatric populations, likely reflecting shared central and peripheral regulatory pathways involving the autonomic nervous system.5,6 These overlapping features may contribute to both dizziness and OI symptoms in pediatric patients with headache. Consequently, OI may be distributed relatively uniformly across different headache subtypes, rather than being specific to a particular diagnostic category. This could be particularly relevant in children and adolescents, in whom clinical phenotypes commonly overlap and are less clearly differentiated than in adults.3,8
In our previous study, we demonstrated that headache-associated symptoms in pediatric migraine are closely related to specific triggering factors, such as sleep disturbance and academic stress, which may significantly influence symptom severity and clinical presentation.11 The present findings extend this concept by showing that even when dizziness is categorized based on underlying mechanisms, such as OI or otologic diseases, its distribution remains independent of headache subtype. Overall, our findings suggest that dizziness in pediatric headaches is a multidimensional symptom influenced by triggering factors, developmental characteristics, and underlying physiological responses.
In contrast, we found that age was significantly associated with both OI and otologic diagnosis. Patients with POTS had the highest mean age, followed by those with OH, while patients without OI were the youngest. This finding is consistent with prior reports indicating that OI and POTS become more prevalent during adolescence, likely reflecting maturational changes in autonomic regulation, cardiovascular adaptation, and hormonal influences.7,12 In addition, rapid somatic growth and pubertal development during adolescence may further contribute to the development of orthostatic symptoms.7 Consequently, the increasing frequency of OI with age may explain the observed differences in mean age across the diagnostic groups.
Similarly, age differences were observed among otologic disease subtypes. Patients with BPVC were the youngest, while those with vestibular neuritis and Ménière’s disease tended to be older. This pattern aligns with known developmental and clinical characteristics of pediatric vestibular disorders. BPVC is typically considered an early life condition, and is often regarded as a precursor to migraine-related disorders, including vM.4,13 In contrast, vestibular neuritis is more commonly observed in older children and adolescents, and may reflect different underlying etiologies, including viral or inflammatory mechanisms.3,8 These findings further support the idea that age plays a critical role in the clinical manifestation of dizziness-related disorders in the pediatric population.
Notably, the frequency of otologic comorbidities was higher in the vM and MwA groups than in the other headache subtypes, although this difference was not statistically significant (p=0.075). This trend may reflect overlapping pathophysiological mechanisms between vM and otologic diseases, particularly Ménière’s disease and BPVC, which share clinical features such as recurrent vertigo and auditory symptoms.13,14 The higher proportion of otologic comorbidities in the vM group further supports the notion that vM in children may be associated with a broader spectrum of vestibular dysfunction. However, given the relatively small sample size in each subgroup, these findings should be interpreted with caution and require validation in larger prospective studies.
Additionally, a significant association was identified between sex and OI, with marked female predominance in the POTS group. This finding is consistent with prior studies reporting a higher proportion of POTS in adolescent females.7,12 Hormonal factors, particularly fluctuations in estrogen levels, as well as sex-related differences in autonomic regulation and vascular responsiveness, have been proposed as contributing mechanisms.6,7 These differences may become more pronounced during puberty, which further supports the observed age-related trends.
Taken together, our findings indicate that OI is common among pediatric patients with headache and dizziness and is not specific to particular headache subtypes. Instead, age and sex appeared to be more important factors influencing the clinical presentation and distribution of OI and otologic diseases. These results have important clinical implications as they highlight the need for a comprehensive and multidisciplinary approach when evaluating pediatric patients with headache and dizziness, rather than relying solely on headache classification.
Nevertheless, this study had several limitations. First, the retrospective design limited the availability of standardized clinical and diagnostic data. Second, this was a single-center study, which may limit the generalizability of the findings to a broader population. Third, not all patients underwent a uniform HUTT, and the diagnostic classifications were based on clinical assessments and available data rather than on standardized protocols. Because HUTT was performed only when clinically indicated, patients with more prominent autonomic symptoms may have been preferentially evaluated, potentially leading to an overestimation of the absolute frequency of OI. Despite this potential bias, the comparative analyses according to headache subtype, age, and sex remain informative within the evaluated cohort. Additionally, the retrospective and cross-sectional nature of this study limited the ability to assess causal relationships, longitudinal changes, and the temporal relationship between headache and dizziness symptoms. Therefore, we were unable to determine whether dizziness preceded headache onset or vice versa.
Conclusion
In the present study, we found that OI was commonly observed in pediatric patients with headache and dizziness but did not differ significantly according to headache subtype. In contrast, age and sex differences indicate distinct clinical patterns, particularly in POTS and other otologic diseases. These findings may help improve the understanding and clinical evaluation of pediatric patients presenting with the overlapping symptoms of headache, dizziness, and OI.
AVAILABILITY OF DATA AND MATERIAL
The data presented in this study are available upon reasonable request from the corresponding author.
AUTHOR CONTRIBUTIONS
Conceptualization: HJS, KHL; Data curation, HJS, KHL; Formal analysis, HJS; Project administration, HJS, KHL; Visualization: HJS; Writing–original draft: HJS, KHL; Writing–review & editing: HJS, KHL.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING STATEMENT
None.
ACKNOWLEDGMENTS
The authors express their gratitude to the participants who participated in the study.
Figure 1.
Distribution of orthostatic intolerance and otologic diseases by headache subtype. (A) Distribution of orthostatic intolerance categories (OH, POTS, and none) across headache subtypes. (B) Proportion of patients with otologic diseases across headache subtypes.
MwoA, migraine without aura; MwA, migraine with aura; vM, vestibular migraine; TTH, tension-type headache; OH, orthostatic hypotension; POTS, postural orthostatic tachycardia syndrome.
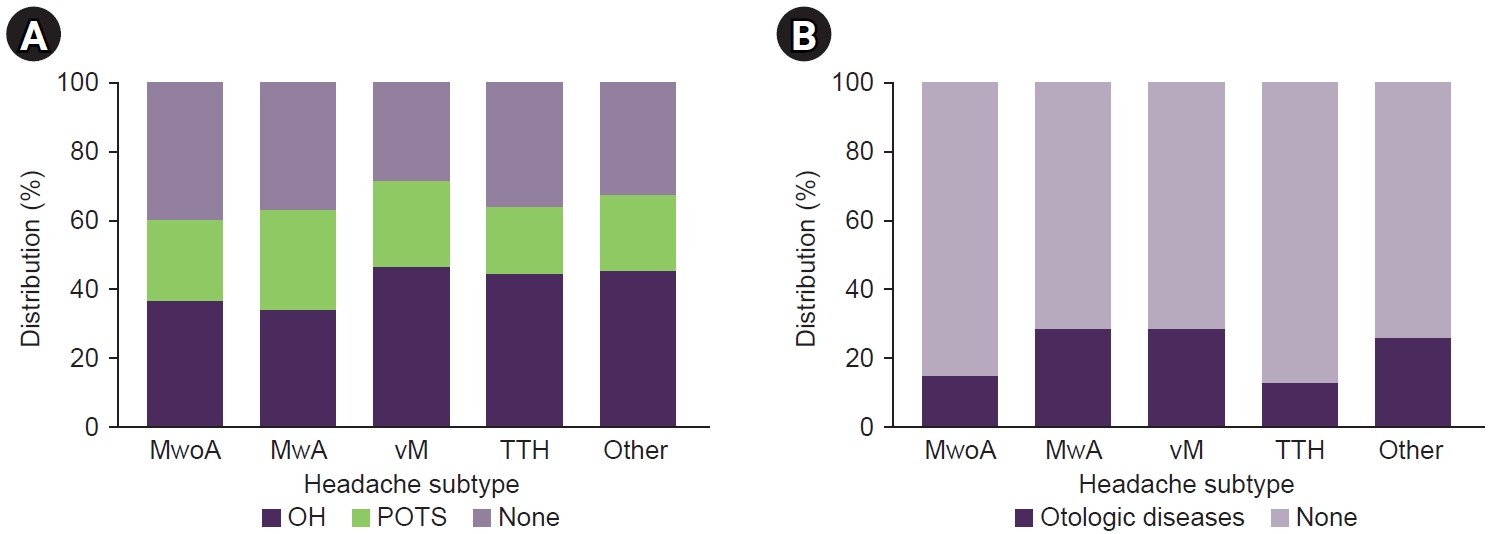
Figure 2.
Age distribution by orthostatic intolerance category and otologic subtype. (A) Age distribution by orthostatic intolerance category (OH, POTS, and none; p<0.001). (B) Age distribution by otologic disease subtype (p=0.003).
OH, orthostatic hypotension; POTS, postural orthostatic tachycardia syndrome; BPPV, benign paroxysmal positional vertigo; BPVC, benign paroxysmal vertigo of childhood.
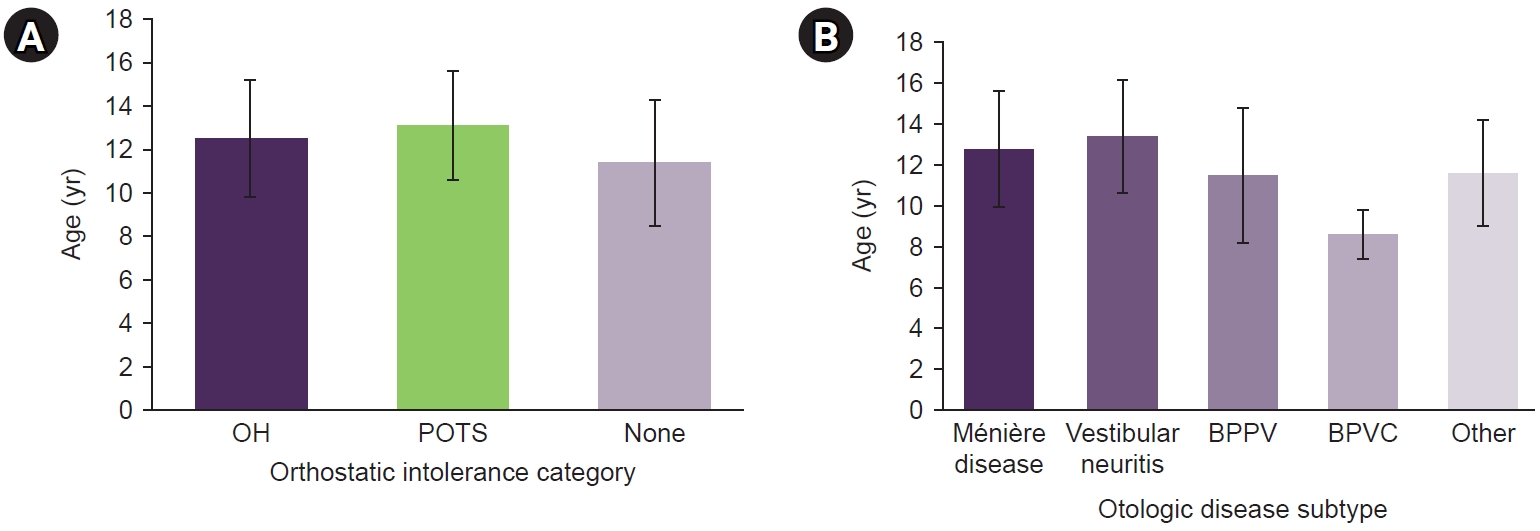
Table 1.Baseline characteristics of patients stratified by headache subtype
|
Variable |
Total (n=310) |
MwoA (n=133) |
MwA (n=35) |
vM (n=49) |
TTH (n=47) |
Other (n=46) |
|
Demographics |
|
|
|
|
|
|
|
Age (yr) |
12.2±2.8 |
12.0±2.7 |
12.5±2.6 |
12.8±2.9 |
12.1±2.8 |
11.9±3.0 |
|
Female sex |
197 (63.5) |
78 (58.6) |
26 (74.3) |
35 (71.4) |
31 (66.0) |
27 (58.7) |
|
Orthostatic intolerance |
|
|
|
|
|
|
|
OH |
126 (40.6) |
49 (36.8) |
12 (34.3) |
23 (46.9) |
21 (44.7) |
21 (45.7) |
|
POTS |
72 (23.2) |
31 (23.3) |
10 (28.6) |
12 (24.5) |
9 (19.1) |
10 (21.7) |
|
None |
112 (36.1) |
53 (39.8) |
13 (37.1) |
14 (28.6) |
17 (36.2) |
15 (32.6) |
|
Otologic diseases |
|
|
|
|
|
|
|
Ménière disease |
18 (5.8) |
5 (3.8) |
3 (8.6) |
4 (8.2) |
2 (4.3) |
4 (8.7) |
|
Vestibular neuritis |
16 (5.2) |
4 (3.0) |
2 (5.7) |
5 (10.2) |
2 (4.3) |
3 (6.5) |
|
BPPV |
10 (3.2) |
3 (2.3) |
1 (2.9) |
2 (4.1) |
1 (2.1) |
3 (6.5) |
|
BPVC |
9 (2.9) |
3 (2.3) |
2 (5.7) |
2 (4.1) |
1 (2.1) |
1 (2.2) |
|
Other otologic diseases |
9 (2.9) |
5 (3.8) |
2 (5.7) |
1 (2.0) |
0 (0.0) |
1 (2.2) |
REFERENCES
- 1. Rho YI, Chung HJ, Lee KH, et al. Prevalence and clinical characteristics of primary headaches among school children in South Korea: a nationwide survey. Headache 2012;52:592-599.Article
- 2. Bisdorff A, Von Brevern M, Lempert T, Newman-Toker DE. Classification of vestibular symptoms: towards an international classification of vestibular disorders. J Vestib Res 2009;19:1-13.ArticlePubMed
- 3. Zhang J, Zhu Q, Shen J, et al. Etiological classification and management of dizziness in children: a systematic review and meta-analysis. Front Neurol 2023;14:1125488.Article
- 4. Gruber M, Cohen-Kerem R, Kaminer M, Shupak A. Vertigo in children and adolescents: characteristics and outcome. ScientificWorldJournal 2012;2012:109624.ArticlePDF
- 5. Qubty W, Kedia S. Dizziness and orthostatic intolerance in pediatric headache patients. Semin Pediatr Neurol 2016;23:71-78.ArticlePubMed
- 6. Wig R, Oakley CB. Dysautonomia and headache in the pediatric population. Headache 2019;59:1582-1588.ArticlePubMedPDF
- 7. Boris JR, Moak JP. Pediatric postural orthostatic tachycardia syndrome: where we stand. Pediatrics 2022;150:e2021054945.ArticlePubMedPDF
- 8. Rey-Berenguel M, Espinosa-Sanchez JM. A practical diagnostic approach to pediatric episodic vestibular syndrome. Children (Basel) 2026;13:583.ArticlePubMedPMC
- 9. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2013;33:1-211.Article
- 10. Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Auton Neurosci 2011;161:46-48.ArticlePubMed
- 11. Son HJ, Jin JO, Lee KH. Evaluation of pediatric migraine triggers: a single-center study. Clin Exp Pediatr 2025;68:163-169.ArticlePubMedPMCPDF
- 12. Cai H, Wang S, Zou R, et al. Comparison of the active sitting test and head-up tilt test for diagnosis of postural tachycardia syndrome in children and adolescents. Front Pediatr 2021;9:691390.ArticlePubMedPMC
- 13. van de Berg R, Widdershoven J, Bisdorff A, et al. Vestibular migraine of childhood and recurrent vertigo of childhood: diagnostic criteria consensus document of the Committee for the Classification of Vestibular Disorders of the Bárány Society and the International Headache Society. J Vestib Res 2021;31:1-9.ArticlePubMedPMC
- 14. Cokyaman T, Cetin H. Pediatric vestibular migraine: diagnosis according to ICHD-3 criteria and the effectiveness of short-term CH prophylaxis. Eur J Paediatr Neurol 2022;39:19-24.ArticlePubMed
Citations
Citations to this article as recorded by


 , Kon-Hee Lee2
, Kon-Hee Lee2
 PubReader
PubReader ePub Link
ePub Link Cite this Article
Cite this Article