
Articles
- Page Path
- HOME > Headache Pain Res > Volume 26(3); 2025 > Article
-
Original Article
Trigeminal Autonomic Cephalalgias Following Unilateral Dorsolateral Medullary Infarction: A Case Series and Literature Review -
Jae-Myung Kim
 , Hak-Loh Lee, You-Ri Kang, Joon-Tae Kim, Seung-Han Lee
, Hak-Loh Lee, You-Ri Kang, Joon-Tae Kim, Seung-Han Lee -
Headache and Pain Research 2025;26(3):218-225.
DOI: https://doi.org/10.62087/hpr.2025.0013
Published online: October 22, 2025
Department of Neurology, Chonnam National University Hospital, Chonnam National University Medical School, Gwangju, Republic of Korea
- Correspondence: Seung-Han Lee, M.D., Ph.D. Department of Neurology, Chonnam National University Hospital, 42 Jebong-ro, Dong-gu, Gwangju 61469, Republic of Korea Tel: +82-62-220-6274, Fax: +82-62-228-3461, E-mail: nrshlee@chonnam.ac.kr
© 2025 The Korean Headache Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,947 Views
- 28 Download
- 1 Crossref
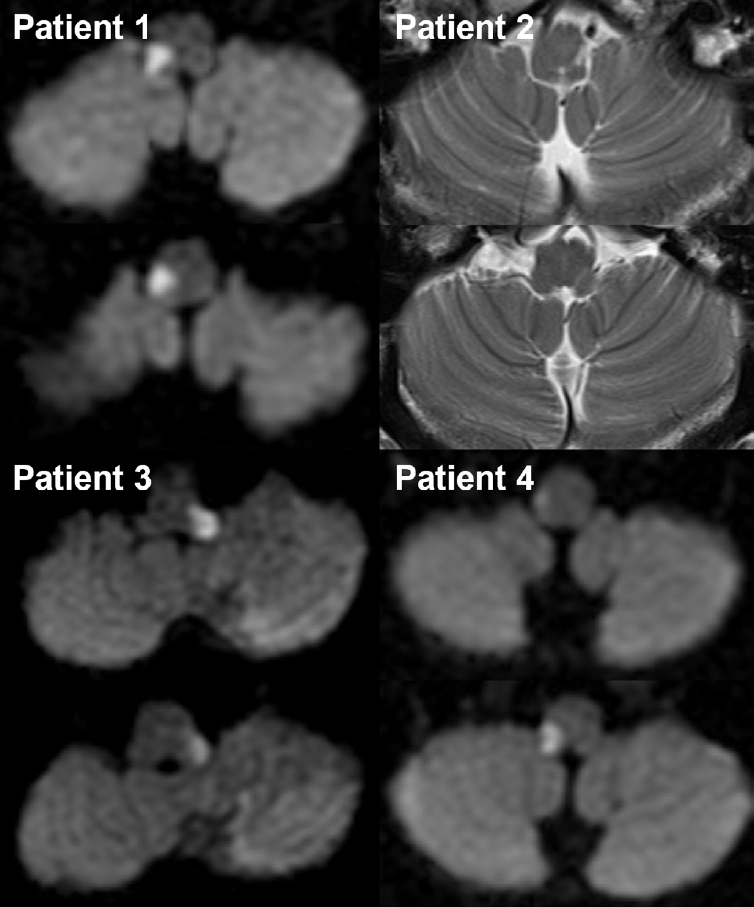
Figure & Data
References
Citations
- Primary or Secondary Headache Disorders in Moyamoya Disease and Cerebral Infarction: Clinical Challenges and the Potential Role of Non-Vasoconstrictive Migraine Therapies
Soo-Jin Cho
Headache and Pain Research.2026; 27(1): 1. CrossRef
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-

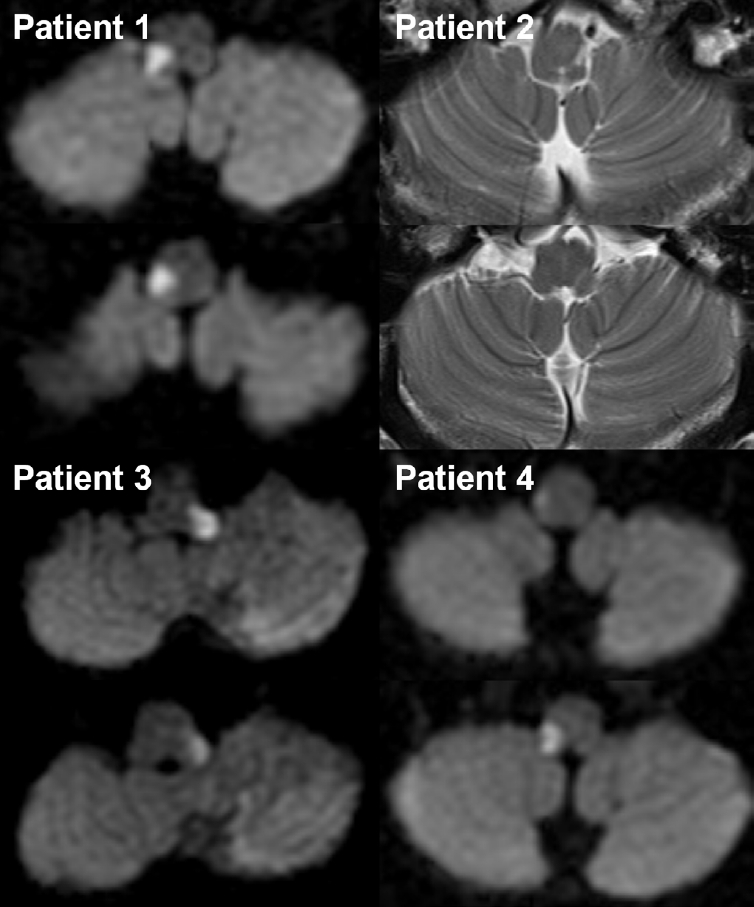
Figure 1.
| SNUHA |
| A. At least 20 attacks fulfilling criteria B–D |
| B. Moderate or severe unilateral head pain, with orbital, supraorbital, temporal, and/or other trigeminal distribution, lasting 1–600 seconds and occurring as single stabs, series of stabs, or in a saw-tooth pattern |
| C. At least one of the following five cranial autonomic symptoms or signs, ipsilateral to the pain: |
| 1. conjunctival injection and/or lacrimation |
| 2. nasal congestion and/or rhinorrhoea |
| 3. eyelid oedema |
| 4. forehead and facial sweating |
| 5. forehead and facial flushing |
| 6. sensation of fullness in the ear |
| 7. miosis and/or ptosis |
| D. Occurring with a frequency of at least once daily |
| E. Not better accounted for by another ICHD-3 diagnosis. |
| SUNCT |
| A. Attacks fulfilling criteria for SNUHA, and criterion B below |
| B. Both of the following are ipsilateral to the pain: |
| 1. conjunctival injection |
| 2. lacrimation (tearing) |
| SUNA |
| A. Attacks fulfilling criteria for SNUHA, and criterion B below |
| B. Only one or neither of conjunctival injection or lacrimation (tearing). |
| Case | Age (yr) | Sex | Index stroke | Headache characteristics | Diagnosis of headache (ICHD-3) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Risk factor | TOAST | Angiography | MRI lesion | Associated neurological signs | Onset after stroke | Side | Location | Duration | Nature | Frequency (times) | Outcome | Autonomic symptoms | ||||
| Present cases | ||||||||||||||||
| Patient 1 | 70 | Male | HTN, DL | SVO | Normal | Rt. LMI | SL (i-F and c-B), AT (i-L and T), hoarseness | 3 mo | i | Periorbital, hemifacial, and temporal | 1–2 min | Stabbing | 3–4/day | Persistent | LC, CI, rhinorrhea | SUNCT |
| Patient 2 | 57 | Male | SVO | VA hypoplasia | Lt. LMI | SL (i-F and c-B), DysP, AT (i-L), vertigo, NY | 2.5 mo | i | Periorbital, hemifacial, and temporal | 1–2 min | Stabbing | 1–5/day | Resolved after several years | LC, CI | SUNCT | |
| Patient 3 | 56 | Male | Lipid | LAA | VA severe stenosis | Lt. LMI | SL (i-F and c-B), AT (T), HS, vertigo, NY | 4 mo | i | Periorbital, hemifacial, and temporal | <1 min | Electric shock-like | 1–5/day | Persistent | LC, CI, nasal congestion | SUNCT |
| Patient 4 | 50 | Female | HTN, HCC, RA | SOD | VA dissection | Rt. LMI | SL (i-F and c-B), AT (i-L and T), HS, vertigo, NY | 2.5 mo | i | Periorbital, hemifacial, and temporal | <1 min | Electric shock-like | 1–5/day | Persistent | LC | SUNA |
| Published cases | ||||||||||||||||
| Rodrigues et al. (2007)12 | 54 | Male | HTN | N/A | N/A | Rt. LMI | SL (i-F and c-B), AT (i-T), DysA | 6 mo | i | Orbital | 20 sec | N/A | >10/hr | Persistent | LC, CI | SUNCT |
| Jin et al. (2016)6 | 64 | Male | HTN, DM | LAA | VA occlusion | Lt. LMI | SL (i-F), HS, AT (i-T), vertigo | 13 day | i | Periorbital | 3–10 sec | Stabbing | 1–4/day | Resolved after 19 days | LC, CI, rhinorrhea | SUNCT |
| Lambru et al. (2017)7 | 58 | Male | HTN | SOD | VA dissection | Rt. LMI (hemorrhagic) | N/A | 21 day | i | Periorbital–temporal radiating to cheek/jaw | 5–20 sec | Stabbing, sharp | 12–15 (up to 50–60)/day | Persistent | LC, CI, ptosis, eyelid edema, rhinorrhea | SUNCT and TN |
| Lei et al. (2020)11 | 44 | Male | None | LAA | VA stenosis | Rt. LMI | SL (i-F and c-B), DysP, DysA, hiccup, hoarseness, HS, AT (i-L and T), hemiparesis (i), NY, vertigo, gag reflex ↓ | 0 day |
i | Hemifacial, temporal, occipital | 10–180 sec | Tearing | >10/day | Resolved after 1 month | LC, CI, nasal congestion | SUNCT |
| Gadah et al. (2025)10 | ~40 | Male | None | N/A | N/A | Rt. LMI | SL (i-F; V1 and V2), hand numbness (i) | 4 day | i | Hemifacial | 1 min | Burning | >4/day | Improved after 1 month, but persisted until 1 year | LC, CI, nasal discharge, facial grimacing with facial edema | SUNCT |
| Total (n=9) | Male (n=8) | SL (i-F)=8 of 9 | 0 day |
i (100%) | Persistent=5, resolved=4 | SUNCT=8, SUNA=1 | ||||||||||
| Group | Case (Ref.) | Headache onset after stroke | Headache duration | Diagnosis | Tx. regimen (max. daily dose) | Duration (mo) | Associated neurological signs |
|---|---|---|---|---|---|---|---|
| Persistent (n=5) | Patient 1 (this study) | 3 mo | Persistent | SUNCT | VER 80 mg/GBP 800 mg/LIT 600 mg/VPA 250 mg | 42/96/66/72 | SL (i-F and c-B), AT (i-L and T), hoarseness |
| Patient 3 (this study) | 4 mo | Persistent | SUNCT | VER 180 mg/AMI 5 mg/GBP 300 mg | 87/90/75 | SL (i-F and c-B), AT (T), HS, vertigo, NY | |
| Patient 4 (this study) | 2.5 mo | Persistent | SUNA | PGB 150 mg/GBP 800 mg | 74/118 | SL (i-F and c-B), AT (i-L and T), HS, vertigo, NY | |
| Rodrigues et al. (2007)12 | 6 mo | Persistent | SUNCT | VER |
N/A | SL (i-F and c-B), AT (i-T), DysA | |
| Lambru et al. (2017)7 | 21 day | Persistent | SUNCT/TN | CBZ 800 mg/OXC 1,350 mg/GBP 900 mg/AMI 40 mg/LTG 50 mg/DLX 30 mg | N/A | N/A | |
| Mean | - | 3.24 mo | - | - | - | ||
| Resolved (n=4) | Patient 2 (this study) | 2.5 mo | Resolved | SUNCT | GBP 400 mg | 60 | SL (i-F and c-B), DysP, AT (i-L), vertigo, NY |
| Jin et al. (2016)6 | 13 day | Resolved | SUNCT | No Tx. | N/A | SL (i-F), HS, AT (i-T), vertigo | |
| Lei et al. (2020)11 | 0 day | Resolved | SUNCT | N/A | N/A | SL (i-F and c-B), DysP, DysA, hiccup, hoarseness, HS, AT (i-L and T), hemiparesis (i), NY, vertigo, gag reflex ↓ | |
| Gadah et al. (2025)10 | 4 day | Resolved | SUNCT | LTG |
12 | SL (i-F; V1 and V2), hand numbness (i) | |
| Mean | - | 0.76 mo | - | - | - |
SUNCT, short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA, short-lasting unilateral neuralgiform with cranial autonomic symptoms; ICHD-3, International Classification of Headache Disorders, third edition; SNUHA, short-lasting unilateral neuralgiform headache attacks.
TAC, trigeminal autonomic cephalalgia; TOAST, Trial of Org 10172 in Acute Stroke Treatment; MRI, magnetic resonance imaging; ICHD-3, International Classification of Headache Disorders, third edition; HTN, hypertension; DL, dyslipidemia; SVO, small vessel occlusion; Rt., right; LMI, lateral medullary infarction; SL, sensory loss; i, ipsilateral; F, face; c, contralateral; B, body; AT, ataxia; L, limb; T, trunk; LC, lacrimation; CI, conjunctival injection; SUNCT, short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; VA, vertebral artery; Lt., left; DysP, dysphagia; NY, nystagmus; LAA, large artery atherosclerosis; HS, Horner’s syndrome; HCC, hepatocellular carcinoma; RA, rheumatoid arthritis; SOD, stroke of other determined etiology; SUNA, short-lasting unilateral neuralgiform with cranial autonomic symptoms; N/A, not available; DysA, dysarthria; DM, diabetes mellitus; TN, trigeminal neuralgia. Same day as stroke onset.
TAC, trigeminal autonomic cephalalgia; Ref., reference; Tx., treatment; max., maximum; SUNCT, short-lasting unilateral neuralgiform headache with conjunctival injection and tearing; VER, verapamil; GBP, gabapentin; LIT, lithium; VPA, valproic acid; SL, sensory loss; i, ipsilateral; F, face; c, contralateral; B, body; AT, ataxia; L, limb; T, trunk; AMI, amitriptyline; HS, Horner’s syndrome; NY, nystagmus; SUNA, short-lasting unilateral neuralgiform with cranial autonomic symptoms; PGB, pregabalin; CBZ, carbamazepine; LTG, lamotrigine; N/A, not available; DysA, dysarthria; OXC, oxcarbazepine; DLX, duloxetine; TN, trigeminal neuralgia; DysP, dysphagia. Exact medication doses were not reported in the original case reports.
Table 1.
Table 2.
Table 3.
TOP

